Download as PDF, PPTX










![Activates assumptions
1. I will perform very poor
2. I am incompetent to present such topic
Perceived social danger
(everybody laugh on me, teacher and
other students will think that I am
stupid)
Processing of Self as a Social
Object (everybody watching
me/ my symptoms and my
single mistake will ruined my
and my families reputation)Safety behaviours
(Avoid going school or
tried to bung the class)
a
Somatic & cognitive
symptoms
(heart beat, respiration,
palpitation mind goes blank,
unable to concentrate, )
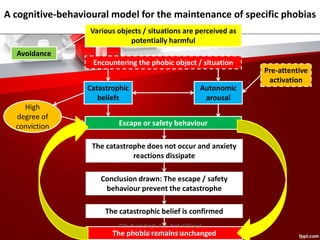
Cognitive Behaviour model of social phobia
[Clarks and Wells (1995) and Wells and Clark (1997)]
Social Situation
Presentation in class
©Dr. Preeti Singh, Asst. Prof of Clinical
Psychology, IMHH, Agra](https://image.slidesharecdn.com/phobiacbtconceptualization-170516153319/85/Phobia-cbt-conceptualization-38-320.jpg)

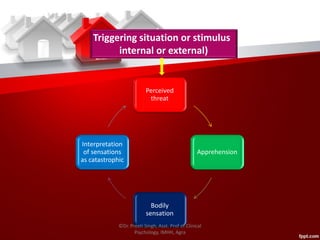


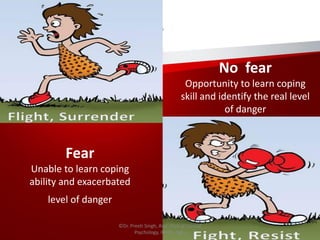
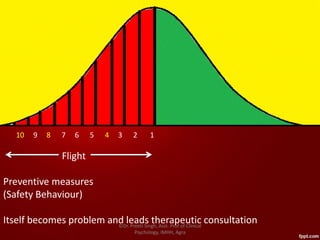
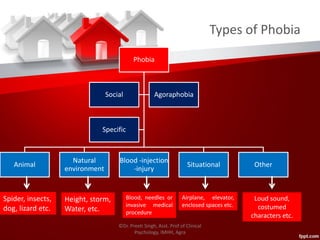
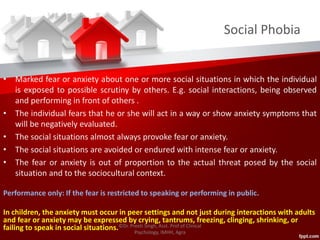
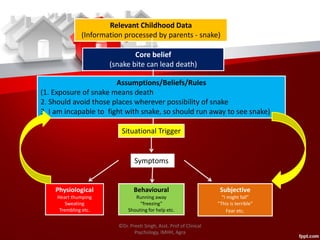
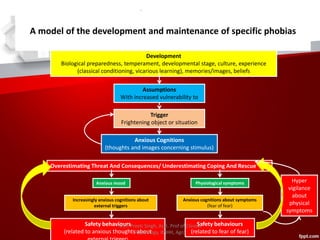
The document provides an overview of conceptualization of phobias from a cognitive behavioral therapy (CBT) perspective. It discusses the distinction between normal fear and phobias. It then covers CBT models of the development and maintenance of specific phobias using cognitive and behavioral factors. Models of social phobia, claustrophobia, and agoraphobia are presented. The document also discusses characteristics of phobias in children, adolescents, adults and older adults as well as differences by gender. Finally, it outlines types of phobias and cognitive and behavioral factors involved in blood-injection-injury phobia and social phobia.



































































