This document discusses strategies for addressing obesity at the national level. It describes trends showing rising obesity rates in many countries over recent decades. Some key points made include:
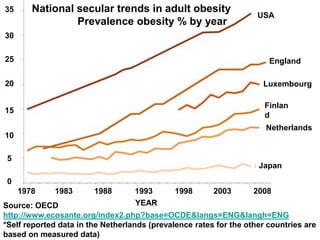
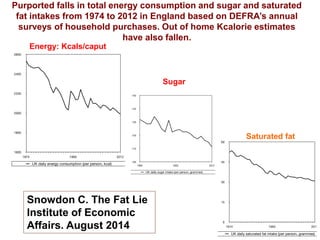
- Obesity rates have risen sharply in countries like the US, England, and Luxembourg since the 1970s.
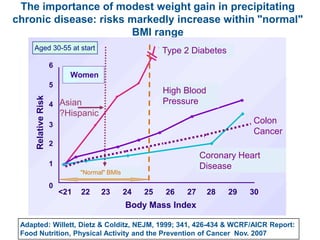
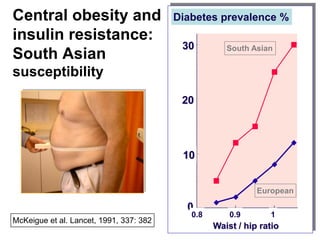
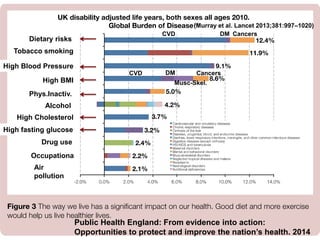
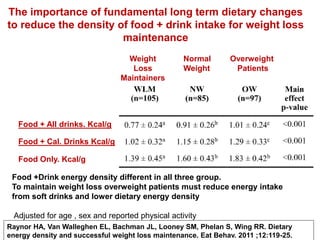
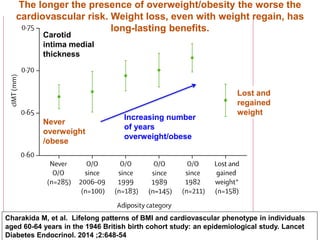
- Modest weight gain, even within the "normal" BMI range, increases risks for chronic diseases.
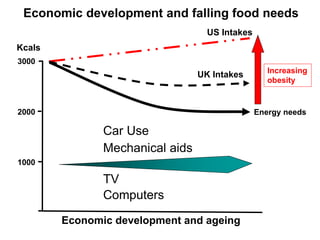
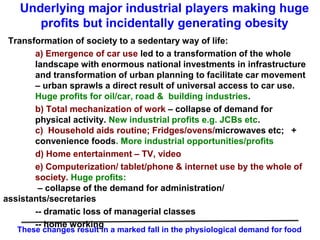
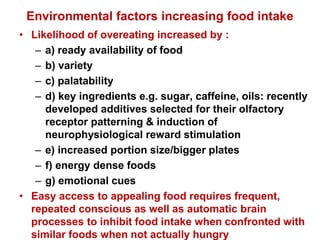
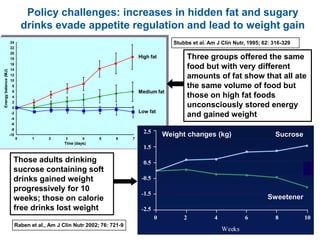
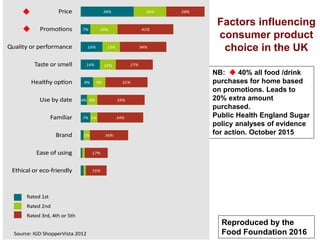
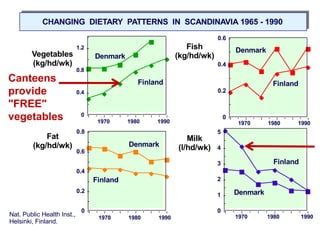
- Environmental factors like increased food availability, variety, and portion sizes can promote overeating.
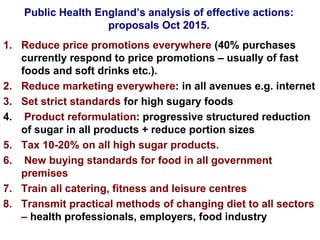
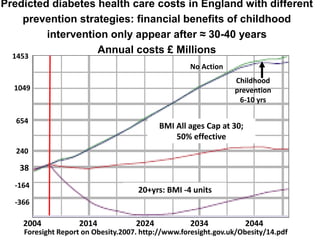
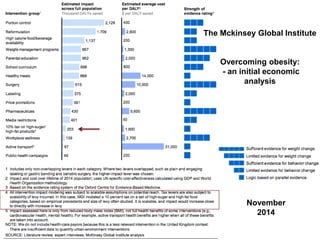
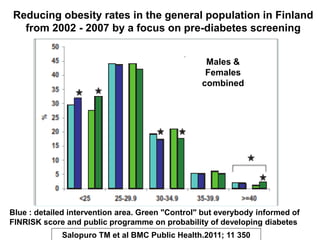
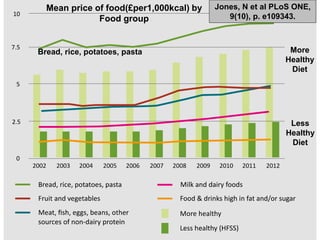
- Population-wide strategies are needed like marketing restrictions, pricing policies, and changing food environments in schools and hospitals.