Downloaded 104 times


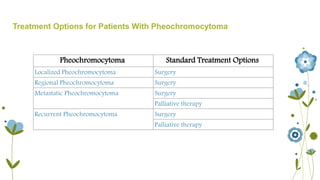


This document discusses the case of a 36-year-old woman presenting with intermittent high blood pressure, sweating, and panic attacks who is suspected of having pheochromocytoma. For initial treatment, alpha blockade with phenoxybenzamine is recommended for at least 1-3 weeks before surgery to prevent hypertensive crisis during the operation. Laparoscopic surgery is preferred for smaller tumors, while larger tumors typically require open surgery. Following successful removal of the tumor, most patients become normotensive, though some may remain hypertensive and require further treatment and monitoring.















![Acute heart failure [MBBS]](https://cdn.slidesharecdn.com/ss_thumbnails/acuteheartfailure-170323061012-thumbnail.jpg?width=640&height=640&fit=bounds)




















































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


















