• Peripheral neuropathiesoccur when there is a generalized dysfunction or disease of many
or all peripheral nerves.
• Based on the characteristics of the neuropathy (axonal, demyelinating, sensory, motor, etc.)
• Fiber that Are Involved: (Motor, Large Sensory, Small Sensory, Autonomic). Determining
which fiber types are involved has important diagnostic implications.
3.
• May behereditary or acquired.
• Most patients with polyneuropathy first present with a combination of sensory and
motor symptoms and signs in the feet and lower legs, which later spread proximally
in the legs and then into the hands and arms.
• Most polyneuropathies are chronic. Acute polyneuropathies are less common
5.
Significance of Electrophysiologicstudies in PN:
• to confirm the presence of a polyneuropathy
• to assess its severity and pattern
• to determine whether motor, sensory, or a combination of fibers are
involved
• to assess whether the underlying pathophysiology is axonal loss or
demyelination.
• In cases in which a demyelinating polyneuropathy is found, further
differentiation between an acquired and inherited condition can often be
made.
6.
What Is theTemporal Course of the Polyneuropathy (Acute,
Subacute, Chronic; Progressive, Stepwise, Relapsing/Remitting)?
• Most polyneuropathies are chronic
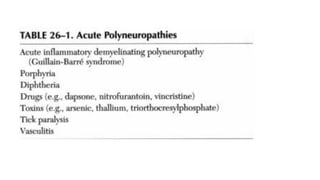
• Acute polyneuropathies are less common, Guillain-Barre syndrome[AIDP] is the most
acute type.
• Polyneuropathies that progress in a stepwise fashion are infrequent and often are
associated with a mononeuropathy multiplex
• relapsing/remitting course is unusual and suggests either an intermittent
exposure/intoxication or a variant of chronic inflammatory demyelinating polyneuropathy
(CIDP)
8.
Which Fiber TypesAre Involved (Motor,
Large Sensory, Small Sensory, Autonomic)?
• This information is obtained primarily from the history and confirmed by
physical examination and electrophysiologic tests.
• Large sensory fibers mediate vibration, proprioception, and touch, whereas
small sensory fibers convey pain and temperature sensations
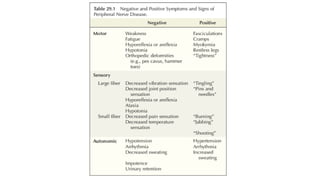
• Symptoms and signs of nerve dysfunction result either from lack of
function (negative symptoms and signs) or from abnormal function or over
functioning (positive symptoms and signs).
11.
What Is thePattern of the Polyneuropathy (Multiple Nerves; Symmetry,
Asymmetry)?
• The overall pattern of the polyneuropathy is determined largely based on
the clinical examination
• In most polyneuropathies, there is a distal-to-proximal gradient of
symptoms and signs.
• the longest nerves are affected first, resulting in a stocking-glove
distribution of symptoms. Patients initially develop numbness or weakness
of the toes and feet, which then slowly progresses up the leg.
• When the process reaches the upper calf, the fingertips become involved
as well (the distance from the lumbosacral spinal cord to the upper calf is
the same as that from the cervical spinal cord to the fingertips).
12.
• Only rarelypolyneuropathies preferentially affect the shorter, more
proximal nerves before the distal ones (e.g., in porphyria, proximal diabetic
neuropathy, and some cases of inflammatory demyelinating
polyneuropathy).
• Nearly all polyneuropathies are symmetric.
• The presence of any asymmetry is a key finding for the possibility of:
➢a mononeuropathy multiplex pattern (vasculitis and vasculitic neuropathy)
➢superimposed radiculopathy or entrapment neuropathy,
➢variant of CIDP.
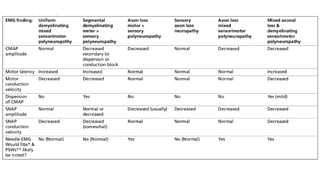
14.
What Is theUnderlying Nerve Pathology
(Axonal, Demyelinating, or Mixed)?
• The vast majority of polyneuropathies are primarily axonal.
• In demyelinating polyneuropathies, the initial injury to the nerves
reflects damage to or dysfunction of the Schwann cells and the
myelin sheaths.
• As a consequence of demyelination, conduction is impaired with
marked slowing of conduction velocity or frank conduction block.
15.
Axonal Loss
• Asaxons are lost, the amplitudes of these potentials decrease. The best way to assess
the amount of axonal loss is to compare the amplitude of a potential with a previous
baseline value, a normal control value, or the contralateral (asymptomatic) side.
• Although axonal loss lesions generally result in reduced amplitudes, the corollary is not
necessarily true.
• Axonal polyneuropathies include nearly all diabetic, toxic, metabolic, drug-induced,
nutritional, connective tissue, and endocrine-associated polyneuropathies.
16.
Demyelination:
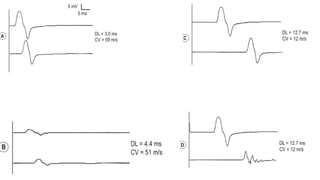
• On NCSs,demyelination is associated with marked slowing of conduction velocity
(slower than 75% of the lower limit of normal), marked prolongation of distal latency
(longer than 130% of the upper limit of normal), or both.
• Any motor, sensory, or mixed nerve conduction velocity that is slower than 35 m/s in
the arms or 30 m/s in the lower limbs signifies unequivocal demyelination.
• A conduction velocity near the cutoff value with a normal amplitude usually represents
demyelination, whereas a borderline velocity with a markedly reduced amplitude most
often implies severe axonal loss.
17.
Conduction Block
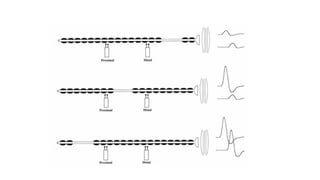
• Theamplitude will be low if the nerve is stimulated proximal to a conduction block.
• If a conduction block is present between the normal distal stimulation site and the
recording electrodes, both the distal and proximal CMAP amplitudes will be low and
may simulate an axonal loss lesion
• If a conduction block is present between distal and proximal stimulation sites, the
CMAP amplitude will be normal distally, below the block, but will be decreased at
the proximal stimulation site, above the block.
• if both the proximal and distal stimulation sites are distal to, or below the block, the
CMAP amplitudes will remain normal both distally and proximally
19.
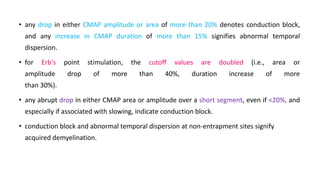
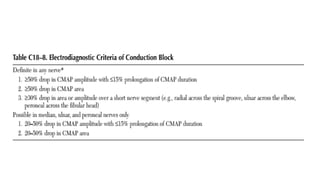
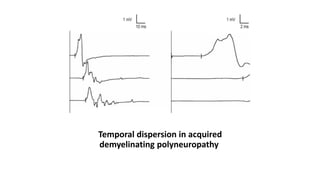
• any dropin either CMAP amplitude or area of more than 20% denotes conduction block,
and any increase in CMAP duration of more than 15% signifies abnormal temporal
dispersion.
• for Erb's point stimulation, the cutoff values are doubled (i.e., area or
amplitude drop of more than 40%, duration increase of more
than 30%).
• any abrupt drop in either CMAP area or amplitude over a short segment, even if <20%, and
especially if associated with slowing, indicate conduction block.
• conduction block and abnormal temporal dispersion at non-entrapment sites signify
acquired demyelination.
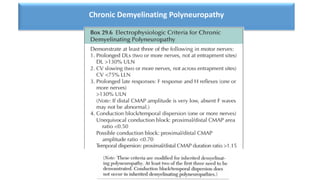
22.
Is There aFamily History of Polyneuropathy?
• Several clinical clues, suggest the possibility of an inherited polyneuropathy:
➢Foot deformity (pes cavus, hammer toes, high arches)
➢History of a long-standing polyneuropathy (many years and often decades)
➢History of very slow progression
➢Few positive sensory symptoms
➢Family history of "polio," “neuropathy," "arthritis," or other disorders that actually might have
been inherited polyneuropathy
23.
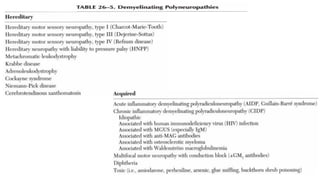
Acquired versus inheriteddemyelinating
polyneuropathies.
• In a patient with an inherited condition, all myelin tends to be affected equally; thus,
uniform slowing of conduction velocity occurs. Accordingly, nerve conduction studies usually
are symmetric from side to side.
• In contrast, acquired conditions (e.g, CIDP) are associated with patchy, often multifocal
demyelination. As a result, asymmetry is found on nerve conduction studies (even in the face
of clinical symmetry), along with evidence of conduction block and temporal dispersion.
• Conduction block and temporal dispersion are key findings for differentiating acquired
from inherited demyelinating polyneuropathies.
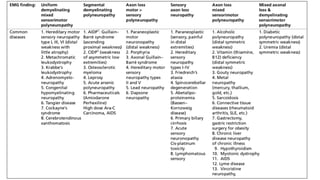
Is There aHistory of Medical Illness Associated with
Polyneuropathy?
• Most prominent among them are diabetes and other endocrine
disorders, cancer, connective tissue disorders, porphyria, vitamin and
other deficiency states, and human immunodeficiency virus (HIV)
infection.
27.
Is There AnyHistory of Occupational or Toxic Exposure to
Agents Associated with Polyneuropathy?
• occupational and exposure history.
• Among drugs, most notable are cancer chemotherapeutic agents,
• alcohol, is one of the most frequent causes of toxic polyneuropathy.
• Lead is one of the most important occupational exposure.
AXONAL POLYNEUROPATHY
• Clinically,the usual axonal polyneuropathy presents with a
stocking-glove distribution of symptoms and signs, including
distal sensory loss and weakness. Ankle reflexes usually are
absent, whereas knee and upper extremity reflexes are preserved,
unless the polyneuropathy is severe.
33.
NCS
• motor andsensory amplitudes decrease, with normal or only
slightly slowed distal latencies, and conduction velocities.
• however, conduction velocity slowing may alternatively indicate severe
axonal loss with dropout of the fastest-conducting fibers. It is in this
situation, when distal CMAP amplitudes are low and conduction velocity
slowing nears 75% of the lower limit of normal.
• The changes are always more marked in the lower extremities, where the
pathology is the greatest
late responses are normal
34.
The Use ofthe Sural/Radial Amplitude Ratio in Mild Polyneuropathy
• The sural/radial amplitude ratio (SRAR) is helpful in those patients with a
borderline normal sural amplitude.
• In the original description of this technique an SRAR <0.40 had a specificity of 90%
and a sensitivity of 90% in detecting an axonal polyneuropathy.
• the SRAR was less dependent on age than the sural amplitude alone and also did
not appear to be affected by body mass index.
• A latter study suggested that a cutoff value of 0.4 may have been too high, and a
more appropriate cutoff should be 0.21. this improved specificity to 95%
35.
Needle EM G
•Denervation typically develops within weeks and reinnervation after weeks to
months.
• If the process is relatively active and progressive, a combination of denervation and
reinnervated motor unit action potentials (MUAPs) with decreased recruitment will
be seen.
• In long-standing and only very slowly progressive, only reinnervated MUAPs with
decreased recruitment will be seen distally, with little or no active denervation
36.
Special Situations inAxonal Polyneuropathy: Acute Presentation
• If the polyneuropathy is very acute and denervation is not yet present, the only abnormality
on needle EMG will be normal-appearing MUAPs with reduced recruitment.
• If an axonal polyneuropathy is subacute , active denervation will also be present. MUAPs again
will be normal in morphology, but with reduced recruitment.
• These two patterns are very unusual in the EMG laboratory because very few
polyneuropathies are acute or subacute, and of the ones that are acute/subacute, most are
associated with demyelination and not axonal loss. Acute axonal polyneuropathies include
those associated with porphyria or vasculitis and those rare cases of GBS that are axonal and
not demyelinating.
37.
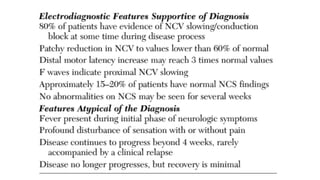
DEMYELINATING POLYNEUROPATHY
several clinicalclues may suggest primary demyelination:
• Global areflexia
• Hypertrophic nerves
• Moderate-to-severe muscle weakness with relative preservation of muscle
bulk
• Motor symptoms and signs more prominent than sensory ones
39.
NCS
• Markedly prolongeddistal latencies (>130% of the upper limit of
normal)
• markedly slowed conduction velocities (usually <75% of the lower
limit of normal)
late responses
• markedly prolonged or absent late responses (>130% of the upper
limit of normal)
40.
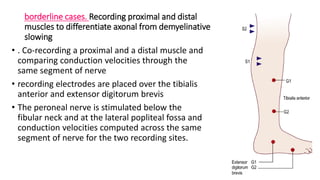
borderline cases. Recordingproximal and distal
muscles to differentiate axonal from demyelinative
slowing
• . Co-recording a proximal and a distal muscle and
comparing conduction velocities through the
same segment of nerve
• recording electrodes are placed over the tibialis
anterior and extensor digitorum brevis
• The peroneal nerve is stimulated below the
fibular neck and at the lateral popliteal fossa and
conduction velocities computed across the same
segment of nerve for the two recording sites.
41.
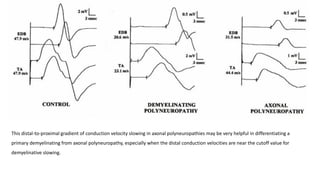
This distal-to-proximal gradientof conduction velocity slowing in axonal polyneuropathies may be very helpful in differentiating a
primary demyelinating from axonal polyneuropathy, especially when the distal conduction velocities are near the cutoff value for
demyelinative slowing.
42.
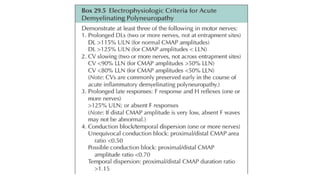
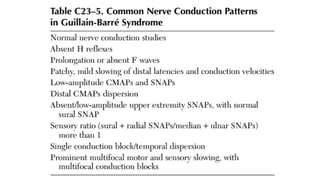
Acute Inflammatory DemyelinatingPolyneuropathy
• is an immune-mediated, rapidly progressive, predominantly
motor polyneuropathy that often leads to bulbar and respiratory
compromise.
• all ages can be affected, although it is most common in young adults.
• An antecedent event, often an upper respiratory infection or
gastroenteritis, is found in approximately 60% of patients.
Prognosis of AIDP
•Low distal CMAP amplitudes «20% of the lower limit of normal at 3-5 weeks)
are the best single predictor of a poor outcome or prolonged course.
• Other nerve conduction and EMG data (including the amount of fibrillation
potentials) actually correlate poorly with prognosis.
• Indeed, some patients have nerve conduction results that appear to worsen
despite clinical improvement. This likely represents the early recovery of fibers
that previously were blocked and now are able to conduct, albeit very slowly.

![What Is the Temporal Course of the Polyneuropathy (Acute,
Subacute, Chronic; Progressive, Stepwise, Relapsing/Remitting)?
• Most polyneuropathies are chronic
• Acute polyneuropathies are less common, Guillain-Barre syndrome[AIDP] is the most
acute type.
• Polyneuropathies that progress in a stepwise fashion are infrequent and often are
associated with a mononeuropathy multiplex
• relapsing/remitting course is unusual and suggests either an intermittent
exposure/intoxication or a variant of chronic inflammatory demyelinating polyneuropathy
(CIDP)](https://image.slidesharecdn.com/peripheralneuropathyncs1-250722193829-cfb48491/85/peripheral-neuropathy-NCs-for-rhematologist-pdf-6-320.jpg)











































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








