Download to read offline

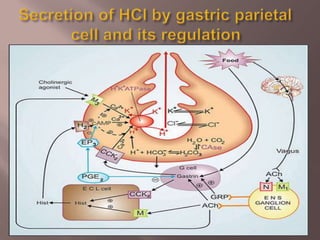


This document summarizes peptic ulcers, which are lesions in the lining of the digestive tract caused by stomach acid. Peptic ulcers occur when there is an imbalance between aggressive factors like H. pylori infection and NSAIDs and the mucosal defenses. Common symptoms include epigastric pain, nausea, and bloody or dark stools. Diagnosis involves tests like endoscopy, blood tests, and breath tests. Treatment options include lifestyle changes, medications to reduce acid secretion, eradicating H. pylori, and sometimes surgery.























































































