–
Pediatric optometry
Pediatric Optometry
isa subspecialty of optometry that is concerned with eye diseases,
visual development, and care in children.
Pediatric Optometry focuses on childhood eye misalignment and
disorders, as well as eye movement prob
The conditions most commonly treated in pediatric optometry are:
1- Refractive errors:
a- Nearsightedness (myopia)
b - farsightedness (hyperopia) and
c - astigmatism
d - Amblyopia (lazy eye)
2 _ Strabismus (misaligned or crossed eyes)
3_ Convergence insufficiency
4_ Eye health issues, such as infection, discharge,
inflammation and injury
5_ Color blindness
2.
Examination Procedures**
A comprehensivepediatric eye and vision examination should
include, but is not limited to:
1- Review of: the nature and history of the presenting problem,
patient and family eye and medical histories, including visual,
ocular, general health,leisure and sports activities, and
developmental and school performance history of the child
2- Measurement of visual acuity
3- Determination of refractive status
• Assessment of binocular vision, ocular motility, and
accommodation
4- • Evaluation of color vision (baseline or if needed, for
qualification purposes or if disease related)
5- • Assessment of ocular and systemic health ,including
evaluation of
a_ pupillary responses
b_ anterior and posterior segment, peripheral retina
c_ /measurement of intraocular pressure and visual field testing.
3.
Patient History
The patienthistory is an initial and ongoing component of the
examination.
The objective is: to obtain
1_ specific information about the patient and/or parent’
s/caregiver’ sperception of the child’ s eye and vision status
2_ important background information on related medicalissues.
- It helps to identify and assess problems,
- it provides an opportunity to become acquainted with the
patient and/or his/her parents or caregivers, establishing a
relationship of confidence and trust.
4.
Major components ofthe patient history include, but are not
limited to:
Nature and history of the presenting problem, including :
1• Visual and ocular history
2• General health history, including
a- prenatal, perinatal and postnatal history,
b- review of systems, surgical and/or head or ocular trauma
history,
c- any vision or ocular treatment
3 • Medication reconciliation, including
a- a- prescription and nonprescription drugs
b- documentation of medication allergies
4 • Family ocular and medical history
5. Clinical note: It is recommended that:- The patient history
should also include the refractive status of bot parent.
6 • Developmental history of the child
5.
7. School performancehistory of school-age children
8 .Time spent outdoors, on sports activities, and on near work
and screen viewing
Visual acuity
Visual acuity is characterized by:
how well child can see from different distances.
For older children who can read, visual acuity
is measured with the same eye chart used in an adult’ s eye
exam.
Babies and small children who can’ t read
are asked to identify different objects and shapes.
The doctor also evaluates a child’ s depth perception
a- their ability to see objects three-dimensionally and
b- judge hownear or far an object is — during the exam.
6.
Pediatric optometrists havea difficult time because of :_
how hard it is to test a child for glasses." "Children are too young
to read the letters."
Fig : examples of charts for VA test in c
Preferential looking visual acuit
7.
Preferential looking methods
areuseful for the assessment of visual acuity in infants and
toddlers.
• Fixation preference test
Fixation preference testing results need to: be interpreted in the
context of all other available information
(e.g., degree and type of anisometropia, frequency and type of
strabismus).
Results of fixation preference testing may be unreliable for
diagnosing amblyopia, particularly secondary to anisometropia;
therefore, monocular visual acuity measurements should be
obtained, if possible.
،• Visual evoked potential (VEP) is an objective method that
can e used to provide an estimate of visual acuity in infant
8.
pupil function
Thepupils’ reactions to light are typically the same
regardless of age, making the test to measure pupil function
the same for babies, older children and adults.
1- Pediatric optometrists will use a flashlight and shine it into each
of child’ s eyes
2- See if each of the pupils responds to the new light by
constricting? Or not.
The inability of one or both pupils to respond to light could indicate
a neurological issue and will likely refer child to a specialist
d to a sp
9.
Eye movement
1- Aneye doctor may ask an older child to watch their flashlight (or
finger)
2- as the doctor moves it up and down, left and right. The doctor
will closely watch the child's eyes to see how easily they''re able to
track a moving object.
Additionally, they evaluate how well the eyes work together to
focus on an object.
For babies and young children,
1- pediatric optometrists will use lights and toys to play with the
child. During this time
2- the eye doctor will observe the child’ s tracking ability and eye
alignmen
3- - In babies can do doll eye maneuver to see eye movement
10.
peripheral vision
Eye doctorsalso evaluate peripheral vision during this time, most
commonly measured using the confrontation visual field test with
older children.
During this test, the eye doctor will start to extend their arm around
the side of the child' 's head and
the child must notify the doctor when they detect the doctor''s
hand in their peripheral vision.
11.
Why is thepediatric eye and visual system different from an
adults?
The brain's visual processing and eye movement control centers
are not fully developed or mature when we are born
. The cells and their functions are developed throughout the first
decade of life
. Because of the immaturity of the child's visual system, disorders
that may have little effect on adult's ability to see can have a
profound and lifelong effect on a child's vision.
Strabismus
is a misalignment of the eyes.
There are many forms of strabismus such as :_
1- esotropia when one eye may be turned in
2-- exotropia when one eye may be turned out.
Eye alignment is normally unsteady at birth, but the eyes should be
straight by 4 months of age.
12.
Any infant whocontinues to show an eye misalignment after 4
months of age or a child who alter acquires strabismus should
have a complete eye examination.
Strabismus can be treated with:_
1- surgery
2- , glasses,
3- eye exercises,
) depending on the degree of strabismus and the cause.
13.
Blocked Tear Ducts
Blockedtear ducts occur in about 6 out of 100 newborns.
1 in 5 newborns has a tear duct that is not fully developed.
The cause of blocked tear ducts:_
is a delay in the opening of the tear ducts inside the nose
. This duct is
the tiny tube that leads from the inner corner of the eye to inside
the nose.
Healthy eyes constantly make tears to keep the eye moist.
Tears normally drain from the tear duct down into the nose.
Eyes can become watery because of :-
1- too many tears or
2- the tear duct is blocked
14.
Amblyopia
Amblyopia is:_ oftenreferred to as lazy eye.
Amblyopia is :_ the medical term for a loss of vision in an
apparently healthy eye. occurs when one eye is weaker than the
other and doesn’t achieve normal visual acuity or function.
_. This occurs in infants and young children if there is an
imbalance of the image received between the two eyes.
An eye imbalance can occur when there is :_
1 _ cataract 2 _ strabismus 3_ ptosis (droop eyelid),
4_ eye injury
5- refractive error that is worse in one eye
_ Amblyopia does not usually have symptoms
is often discovered at:_. a school vision screening.
15.
Amblyopia is difficultto diagnose since the child relies on their
‘good’ eye and may be unaware of their problem
•
Signs to watch for:
• Difficulty reading/doing math/playing sports
• Difficulty with attention and focus
• Frequently closing one eye
• Frequent eye rubbing
Ideally, it is treated by:_
an eye doctor before the child is 6 to 10 years old or the vision
loss will be permanent.
. Treatment entails correcting the underlying problem and
encouraging the child to use the lazy eye wearing glasses and/or
wearing a patch over the"good"eye or by instilling an eyedrop to the
good eye.
16.
What Are RefractiveErrors?
• Refractive errors are a common cause of blurred vision.
• They happen when the shape of the eye changes and fails to bend the
light entering the eye correctly.
almost 20% of children under 18 have a diagnosed eye condition.
• During a child’s early years it’s crucial to care for their eyes, which are
rapidly growing and developing.
• Diagnosing eye problems early can help minimize potential damage
and makes treatment faster and more effective
Types of Refractive Errors in child
• There are four common types of refractive errors:
• Myopia, _ sometimes called nearsightedness, makes far-away
objects look blurry
• Hyperopia_ , sometimes called farsightedness, can make nearby
objects look blurry
• Astigmatism _ makes far-away and nearby objects look blurry
17.
Symptoms of RefractiveErrors
• Blurry vision is just one symptom of refractive errors. Others include:
• Double vision
• Hazy vision
• Seeing halos around lights
• Squinting
• Headaches
• Eyes that feel sore or tired . Trouble focusing while reading or
at a computer
• causes hyperopia:
Hyperopia results from one of several causes:
• The eyeball is shorter than normal
• The cornea is less curved than normal
• The lens is thinner than normal
• different causes of astigmatism:
18.
Regular corneal astigmatismis :_
typically genetic, and the most common type of astigmatism.
Irregular corneal astigmatism:_
• may result from:
– An eye injury
– Certain eye surgeries
– Keratoconus– an ocular disease that causes thinning of the
cornea.
• Lenticular astigmatism is caused by an irregular curvature of the
eye lens
causes myopia:
myopia results from one of several causes:
• The eyeball is longer than normal
• The cornea is more curved than normal
• The lens is thicker than normal
19.
• test by:_
• using either retinoscopy or an auto-refractor — shining a light into the
eyes to observe how the light bends as it travels through the cornea
and lens to retina.
• This will give them an initial sense of whether there is a refractive error,
and a rough estimate of the extent of that error.
• using a trial frame or phoropter head and multiple choices of lenses, to
achieve an exact measurement of your optical prescription
• These tests are meant to help your eye doctor evaluate whether you
have a refractive error and what optical prescription will be best to
correct it.
cycloplegic refraction:
Cycloplegic eye drops will cause your pupils to dilate, and prevent you
from over-focusing during your eye exam.
20.
Treatments for RefractiveErrors:_
• Eyeglasses.
• Your optometrist will prescribe an eyeglass lens to correct the
refractive error and help you see clearly.
• Contact lenses
• . Like eyeglasses
• , contact lenses will correct the way light enters your eye. They sit on
the surface of your eye, and show patient how to use them.
• Surgery
• . Some types of laser eye surgery can change the shape of your
cornea and correct your refractive error.
• There are also non-laser surgery options for certain refractive errors
21.
Refractive Error
• Averagerefractive error for a full-term baby = +2.00 D
• Astigmatism present in 50% of newborns
• Average axial length for full-term newborn = 16 mm
• Premature Infants (born<37 weeks) typically have:
-High myopia
-High astigmatism
-Anisometropia
-Often have a normal emmetropization with similar levels of hyperopia
and astigmatism by 12 mo.
• At 10 weeks: mean refractive error = +0.00 to +4.00 D
– (emmetropization decreases hyperopia, reaching +0.00 to +3.00
by 20 weeks
• At 12 months: mean refractive error is +0.50 D – +1.00 D
– remains stable until teen years
• Astigmatism
– At 6 mo: ave = -2.00 D ATR astig
– At 2 yrs: ave = -0.50 D or less (decreases)
22.
– Color Vision
–Newborns to 3 mo:
– can only discriminate between red and achromatic stimuli.
– 3 to 4 mo: _
– ability to discriminate all hues
– 4 to 7 mo:_
– : scotopic sensitivity curve in infants reaches adult levels
– Accommodation and Convergence
– Accommodation and convergence become linked after 2 mo
– (once infant can make consistent convergence)
23.
Keratoconus
• Roughly haveblurry vision in one or both eyes due to bulging of the
cornea
• . This eye disease classically progresses during adolescence into the
20s.
• Signs and symptoms of keratoconus may change as the disease
prgresses. They include:
1- Blurred or distorted vision
• 2- Increased sensitivity to bright light and glare
• 3 - A need for frequent cha ges in eyeglass prescriptions
• 4- Sudden worsening or clouding of vision
• 5- Patient should be examined if patient eyesight is worsening rapidly,
which might be caused by an irregular curvature of the eye
(astigmatism).
24.
Causes
• genetic andenvironmental factors are thought to be involved.
• Around 1 in 10 people with keratoconus also have a parent with the
condition.
•
• Risk factors:
• Having a family history of keratoconus
• Rubbing your eyes vigorously
• Having certain conditions, such as retinitis pigmentosa, Down
syndrome, hay fever and asthma
•
• Complications
• In some situations, :_
• patient cornea may swell quickly and cause sudden reduced vision and
scarring of the cornea.
• This is caused by:_
• a_. a condition in which the inside lining of patient cornea breaks
down, allowing fluid to enter the cornea (hydrops).
• b_. The swelling usually subsides by itself, but a scar may form that
affects patient vision.
25.
• Advanced keratoconus
•also may cause patient cornea to become scarred, particularly where
the cone is most prominent.
• A scarred cornea causes worsening vision problems and may require
cornea transplant surgery.
• In the early stages of keratoconus
• , patient might be able to correct vision problems with glasses or soft
contact lenses.
• Later, patient may have to be fitted with rigid, gas permeable contact
lenses or other types of lenses, such as scleral lenses
• . If the condition progresses to an advanced stage, patient may need a
cornea transplant.
26.
• Anew treatment
•called corneal collagen cross-linking may help to slow or stop
keratoconus from progressing, , possibly preventing the need for a
future cornea transplant.
• This treatment may be offered in addition to the vision correction
options above.
Binocular vision dysfunction (BVD
• BVD is caused by the two eyes not working together, due to a
misalignment between the two eyes.
Signs to watch for:
• Anxiety, Dizziness
• Double vision,Headache
• Light sensitivity,Motion sickness
27.
4. Convergence insufficiency
isa binocular vision conditionthat affects eye muscle coordination and near
vision. It occurs when the eyes aren’t able to effectively work together to
focus on a near object.
Signs to watch for:
• Attention and concentration difficulties
• Blurred vision, Double vision
• Fatigue, especially when reading
• Headaches ,Homework avoidance
• Seeing words move or jump on the page
Nystagmus
: is a congenital or acquired condition characterized by quick, involuntary
back-and-forth eye movements
• . Congenital nystagmus appears in the first few months of life,
• acquired nystagmus appears after 6 months.
• Signs to watch for: Eyes that :_
repetitively and rapidly move from side to side, up and down, or in a ci
28.
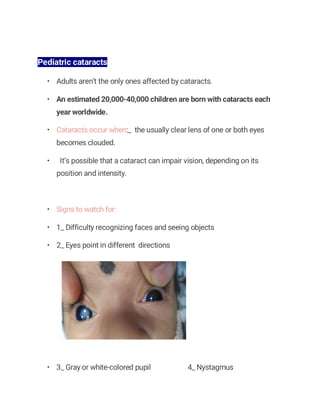
Pediatric cataracts
• Adultsaren’t the only ones affected by cataracts.
• An estimated 20,000-40,000 children are born with cataracts each
year worldwide.
• Cataracts occur when:_ the usually clear lens of one or both eyes
becomes clouded.
• It’s possible that a cataract can impair vision, depending on its
position and intensity.
• Signs to watch for:
• 1_ Difficulty recognizing faces and seeing objects
• 2_ Eyes point in different directions
• 3_ Gray or white-colored pupil 4_ Nystagmus
29.
• 1_ Measlesor rubella —most common cause
• 2_ Genetics,Metabolic problems, Diabetes
• 3 _Trauma
• 4_ Drug reaction to antibiotics, such as tetracycline
Congenital cataracts require:_ early intervention
to prevent the development of other vision problems such as amblyopia, or
“lazy eye”.
(Lazy eye causes eye misalignment and reduced vision, which can impact a
child’s learning ability, appearance, and self esteem.)
The density and location of the cataract will determine:_ the appropriate
treatment plan.
If the cataract is severe,:_ surgery during infancy will be recommended to :_
1- restore normal vision development and
2- prevent vision problems such as amblyopia.
Other treatments,___ with or without surgery, include eyeglasses, contact
lenses, bifocals, and eye-patching
30.
Retinoblastoma
• Retinoblastoma isa rare form of ocular cancer that occurs in 1 in
14,000 – 18,000 live births.
• Retinoblastomas represent 3% of all childhood malignancies.
• Two-thirds are diagnosed before age two, and 95% before age five.
• In many cases, the first sign of the cancer is:_
• 1_ a cross-eyed appearance or
• 2_ one or both pupils appear white instead of red in pictures
• ( While there are many reasons for pupils to appear white in flash
photographs, this cancer should be ruled out through a thorough eye
exam.)
• If a tumor is discovered, the eye is generally removed.
• It is important to note that :_
this form of cancer is highly inheritable— if retinoblastoma runs in the
family, it is crucial to bring your child for regular eye exams to ensure
monitoring of healthy ocular development.
31.
Strabismus
• Strabismus occurswhen the eyes are turned, misaligned or
“crossed.” If left untreated,
• it can lead to amblyopia and permanent vision loss.
• An eye turn might be noticed soon after birth or even suddenly
appear at about two years of age.
• Signs to watch for:
• An eye that points inward, outward, upward or downward
• Excessive and frequent squinting, especially in bright light
• Head tilting, in an effort to align the eyes
32.
causes strabismus:
• Strabismusoften develops in infants and young children, though it
can develop in adults as well.
The condition can be caused by:
• Poor development of eye coordination (binocular vision)
• Severe farsightedness (hyperopia)
• Lazy eye (amblyopia)
• Significant difference of optical prescription between the two eyes
• An ocular muscle weakness (eye movement problems)
• Head trauma or stroke
• Brain tumors or other systemic health issues
33.
signs and symptomsof strabismus:
• Strabismus may initially cause double vision that can be quite
uncomfortable.
• To prevent double vision, the brain begins to actively ignore visual
input from the affected eye, often resulting in amblyopia (lazy eye) or
an eye turn, where the eyes are no longer aligned.
• The most common sign of strabismus is a noticeable misalignment
of the eyes, where one eye is turned up, down, in, or out, when
compared to the other.
• Other symptoms can include:
• Headaches,
• Eye strain
• Double vision
• Reading difficulty or fatigue
34.
• Strabismus treatmentoptions depend on :-
• the type of strabismus—
• direction of eye turns,
• angle of deviations, the presence of convergence
insufficiency, double vision, or amblyopia (lazy eye), etc.
• Treatment
• Non-surgical treatment such as
• glasses,
• prisms,
• and vision therapy are available,
and can lead to improved vision and eye alignment.
• Eye muscle surgery
• may help to ,
• however, the surgery cannot restore the connection between the
eyes and the brain which is vital for vision
35.
Retinopathy of prematurity(ROP)
• also called retrolental fibroplasia (RLF) and Terry syndrome,
• is an eye disease that affects premature babies whose retinal blood
cells have not had the chance to fully develop in utero— leading to
one of the primary causes of ROP: the growth of abnormal retinal
cells.
• These premature infants are given oxygen;-
to support their breathing as their lungs continue to develop outside the
womb— another causative factor in the development of ROP,
as it can also result in the growth of abnormal retinal blood cells.
This condition usually develops in both eyes, and can lead to:-
vision loss and total blindness, if left untreated
36.
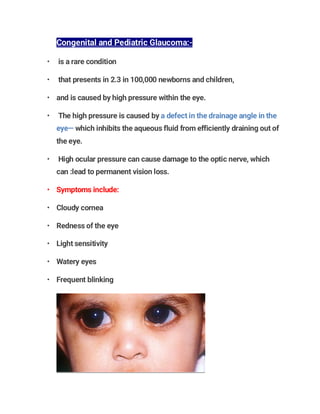
Congenital and PediatricGlaucoma:-
• is a rare condition
• that presents in 2.3 in 100,000 newborns and children,
• and is caused by high pressure within the eye.
• The high pressure is caused by a defect in the drainage angle in the
eye— which inhibits the aqueous fluid from efficiently draining out of
the eye.
• High ocular pressure can cause damage to the optic nerve, which
can :lead to permanent vision loss.
• Symptoms include:
• Cloudy cornea
• Redness of the eye
• Light sensitivity
• Watery eyes
• Frequent blinking
37.
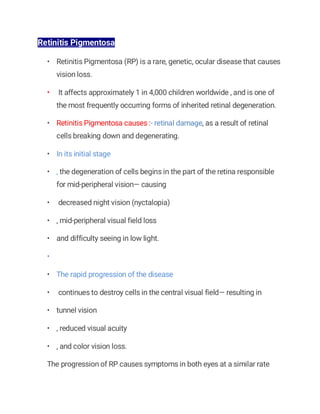
Retinitis Pigmentosa
• RetinitisPigmentosa (RP) is a rare, genetic, ocular disease that causes
vision loss.
• It affects approximately 1 in 4,000 children worldwide , and is one of
the most frequently occurring forms of inherited retinal degeneration.
• Retinitis Pigmentosa causes :- retinal damage, as a result of retinal
cells breaking down and degenerating.
• In its initial stage
• , the degeneration of cells begins in the part of the retina responsible
for mid-peripheral vision— causing
• decreased night vision (nyctalopia)
• , mid-peripheral visual field loss
• and difficulty seeing in low light.
•
• The rapid progression of the disease
• continues to destroy cells in the central visual field— resulting in
• tunnel vision
• , reduced visual acuity
• , and color vision loss.
The progression of RP causes symptoms in both eyes at a similar rate
38.
• in itslater stages, RP causes
• sensitivity to bright lights due to the appearance of an intense glare
(photophobia) and
• the appearance of blinking, shimmering, or swirling lights in the visual
field (photopsia).
• Symptoms of RP typically present in childhood:
• Difficulty seeing at night
• Difficulty adjusting to changes in light
• Sensitivity to bright lights (photophobia)
• Decreased peripheral vision that leads to tunnel vision
• Decreased vision acuity
• Decreased color vision
• Frequently tripping and falling
• Photopsia (blinking/swirling/shimmering lights)
• Blurring of vision
• Poor color separation
• Loss of central vision
• Eventual blindness
39.
• Since RPcan occur from a number of gene mutations, its progression
can differ from person to person
• in some cases,
• central vision is not affected until the person reaches 50 years
• , while in other cases,
• people experience significant loss of vision in early adulthood.
Ultimately, most individuals with RP will lose a significant amount of
their visio
• Many parents of children with RP become concerned as to when their
child might require the support of a cane or guide dog.
40.
treatment of RP
•There is currently no cure for RP.
• 1- When children are first diagnosed with RP :- , they are typically
referred to a low vision specialist for further evaluation.
•
• 2- Many children benefit from low vision aids that aim to ;-
a- magnify existing central vision to widen the field of view and
b- eliminate glare.
•
• 3- A number of low vision devices have been designed to support
children and adults with RP ;-
• Computer programs designed to read text
• Televisions that display text
• Portable lighting devices to enable comfortable lighting for vision
• Mobility training for the use of a cane or guide dog
• Eye scanning to optimize existing vision
• Regular eye examinations will enable proper assessments of the
progression of RP, and will facilitate informed decisions about low
vision services
41.
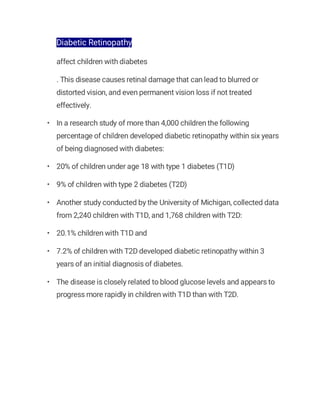
Diabetic Retinopathy
affect childrenwith diabetes
. This disease causes retinal damage that can lead to blurred or
distorted vision, and even permanent vision loss if not treated
effectively.
• In a research study of more than 4,000 children the following
percentage of children developed diabetic retinopathy within six years
of being diagnosed with diabetes:
• 20% of children under age 18 with type 1 diabetes (T1D)
• 9% of children with type 2 diabetes (T2D)
• Another study conducted by the University of Michigan, collected data
from 2,240 children with T1D, and 1,768 children with T2D:
• 20.1% children with T1D and
• 7.2% of children with T2D developed diabetic retinopathy within 3
years of an initial diagnosis of diabetes.
• The disease is closely related to blood glucose levels and appears to
progress more rapidly in children with T1D than with T2D.
42.
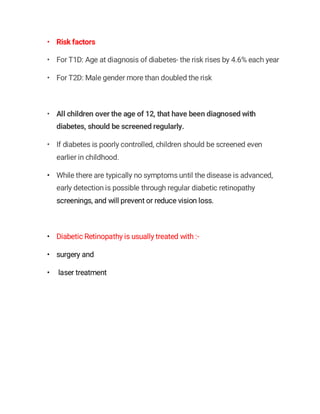
• Risk factors
•For T1D: Age at diagnosis of diabetes- the risk rises by 4.6% each year
• For T2D: Male gender more than doubled the risk
• All children over the age of 12, that have been diagnosed with
diabetes, should be screened regularly.
• If diabetes is poorly controlled, children should be screened even
earlier in childhood.
• While there are typically no symptoms until the disease is advanced,
early detection is possible through regular diabetic retinopathy
screenings, and will prevent or reduce vision loss.
• Diabetic Retinopathy is usually treated with :-
• surgery and
• laser treatment
43.
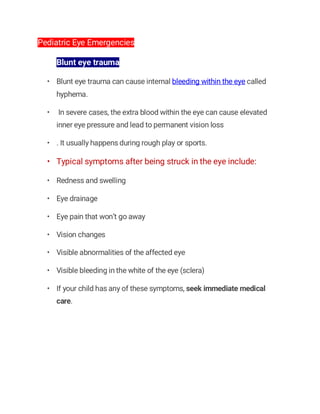
Pediatric Eye Emergencies
Blunteye trauma
• Blunt eye trauma can cause internal bleeding within the eye called
hyphema.
• In severe cases, the extra blood within the eye can cause elevated
inner eye pressure and lead to permanent vision loss
• . It usually happens during rough play or sports.
• Typical symptoms after being struck in the eye include:
• Redness and swelling
• Eye drainage
• Eye pain that won’t go away
• Vision changes
• Visible abnormalities of the affected eye
• Visible bleeding in the white of the eye (sclera)
• If your child has any of these symptoms, seek immediate medical
care.
44.
• chemical exposureto the eye
• A variety of household cleaning products can damage a child’s eyes
and result in an eye care emergency.
• To protect your child’s eyes, keep these things locked away and out of
reach.
• If a child’s eye is exposed to a chemical:-
• 1- look for a phone number on the product’s label to dial in the event of
an emergency or contact your nearest pediatric emergency eye care
department.
• 2- Immediately after the incident:
• Hold your child’s eye open for about 20 minutes while you flush the
eye area with clean water or saline drops.
• If both eyes have been exposed, place your child in the shower and
have them face the water so it goes into their eyes.
45.
cuts or scrapesto the eye
• Particles of dust, sand, wood shavings and other tiny objects can get
into a child’s eye and cause a scratch on the surface of the eye, called
a corneal abrasion.
• Corneal abrasions may cause:
• Vision problems
• Stinging
• Burning
• Light sensitivity
• Red eyes
• Swollen eyes
• Grittiness
• Watery eyes
• If you suspect that your child has a corneal abrasion, immediately
contact an eye doctor near you for treatment.
46.
• Corneal abrasions
•are typically treated with
• eye drops , medicated ointments,
• and sometimes pain relievers.
• To get the object or particle out of the child’s eye,
• rinse the affected eye with saline solution or clean tap water
• They can also blink several times to try and flush out whatever is
scratching the eye
• . Avoid rubbing the eye, as that can make almost any eye condition
worse.
•
• Foreign objects stuck in the eye
• If your child is complaining that something is stuck in their eye,
• the first thing to do is to tell them not to rub their eyes.
• Visually inspect their eyes and see if you find anything
• . If a foreign object is on the sclera, the white part of the eye, try
flushing the eye with saline solution or clean water.
• If it looks like something is lodged in the eye or has penetrated the
eyeball, do not try and remove it. Seek pediatric eye care immediately.
47.
A Guide toEye Infections:
Eye infections can be serious and may cause permanent vision loss.
Effective treatment is always needed, especially when bacteria,
viruses, or fungi invade the eye or the surrounding areas.
The most common eye infections that affect children are called
Viral and Bacterial Conjunctivitis— both highly contagious.
How do you know if child has an eye infection?
Common signs and symptoms:
• Discharge that is green, yellow, or bloody
• Eyelids that are stuck together after waking from sleep
• Red eyes or eyelids
• Feeling that something is stuck in the eye
• Eye pain
• A white or gray sore on the iris
• Increased sensitivity to light
• Sudden blurry vision
• Fever, with no other cause
48.
What causes aneye infection?
• 1) Bacterial conjunctivitis:- a highly contagious, bacterial eye
infection.
• Eyelids are stuck together upon waking in the morning or after a nap
• Presence of yellow or green discharge
• Whites of the eyes may be pink or red
• Eyelids are often swollen
• Affects one or both eye
2-Viral conjunctivitis (pink eye) :- is a highly contagious, viral eye
infection.
• Generally affects both eyes
• Eyes appear pink and watery
• Itchy eyes
• Typically no sign of discharge
• Can appear with a fever, sore throat, and/or runny nose
• Pink eye usually resolves in three to seven days without any treatment
and is no longer contagious once the tearing has stopped.
• Ice packs or artificial tears may alleviate some of the discomfort.
49.
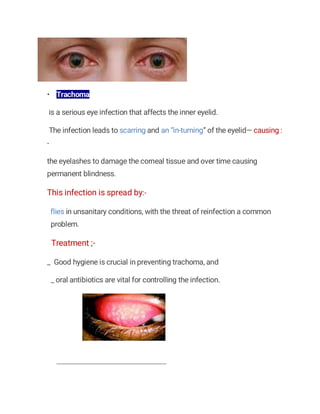
• Trachoma
is aserious eye infection that affects the inner eyelid.
The infection leads to scarring and an “in-turning” of the eyelid— causing :
-
the eyelashes to damage the corneal tissue and over time causing
permanent blindness.
This infection is spread by:-
flies in unsanitary conditions, with the threat of reinfection a common
problem.
Treatment ;-
_ Good hygiene is crucial in preventing trachoma, and
_ oral antibiotics are vital for controlling the infection.
50.
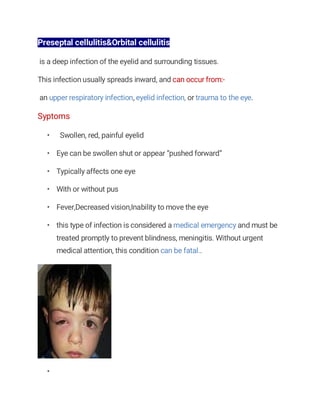
Preseptal cellulitis&Orbital cellulitis
isa deep infection of the eyelid and surrounding tissues.
This infection usually spreads inward, and can occur from:-
an upper respiratory infection, eyelid infection, or trauma to the eye.
Syptoms
• Swollen, red, painful eyelid
• Eye can be swollen shut or appear “pushed forward”
• Typically affects one eye
• With or without pus
• Fever,Decreased vision,Inability to move the eye
• this type of infection is considered a medical emergency and must be
treated promptly to prevent blindness, meningitis. Without urgent
medical attention, this condition can be fatal..
•
51.
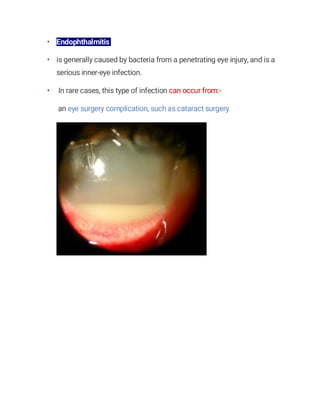
• Endophthalmitis
• isgenerally caused by bacteria from a penetrating eye injury, and is a
serious inner-eye infection.
• In rare cases, this type of infection can occur from:-
an eye surgery complication, such as cataract surgery
52.
corneal ulcer
ypically presentsitself as :- a red, painful eye with some discharge.
_ If not treated promptly, this type of eye problem can lead to
vision loss.
Most often, a corneal ulcer is caused by :-
1- an infection of the cornea after an injury of the eye.
2- Someone who wears contact lenses has a higher risk of this
condition.
3- Severe Dry Eyes
4- ,Allergies ,General Infection,
5- Poor Contact Lens Hygiene
6- Acanthamoeba,
7- Fungus Infection,
8- Ocular Herpes
53.
Eye infections: Causes,symptoms and treatment
• eye infection can happen when bacteria, viruses or fungi invade part
of the eye or its surrounding area. This includes cornea and the
conjunctiva.
• Many eye infections go away on their own or with simple treatment.
• Less commonly, an eye infection can be very serious and require
immediate medical attention
Eye infection symptoms
• Red eyes
• Eye pain
• Eye discharge
• Watery eyes
• Dry eyes
• Light sensitivity
• Swollen eyes
• Swelling around the eyes
• Itching
• Pink eye
54.
• One ofthe most common types of eye infection is conjunctivitis,
more commonly known as pink eye.
Pink eye
is a very contagious eye infection often spread among children in
classrooms and similar environments
Teachers have an increased risk of pink eye when they work in close
quarters with young children.
• Infectious conjunctivitis types are often viral or bacterial.
• Infants can acquire conjunctival eye infections
• (gonococcal and chlamydial conjunctivitis) during birth when
a mother has a sexually transmitted disease.
Besides common pink eye, other viral eye infections include ocular herpes,
_ which occurs with exposure to the Herpes simplex virus
55.
• Stye
• Astye is a common infection that causes a tender, red bump on the
edge of the eyelid.
Styes happen when :-
something blocks an eyelid oil gland,
leading to:- a small, but uncomfortable, bacterial infection
Treatment
. Most styes can be treated using basic home remedies.
In less common situations, they can require medical attention
56.
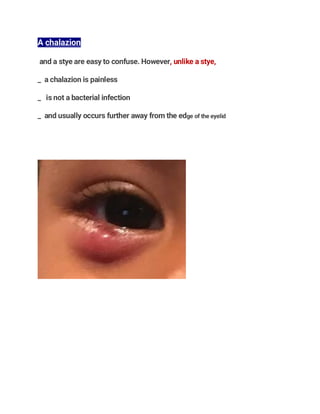
A chalazion
and astye are easy to confuse. However, unlike a stye,
_ a chalazion is painless
_ is not a bacterial infection
_ and usually occurs further away from the edge of the eyelid




































![OCULAR EMERGENCIES IN PEDIATRICS [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ocularemergenciesinpediatricsautosaved-240430020133-f6bf2643-thumbnail.jpg?width=640&height=640&fit=bounds)






































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




