Def: whatthe drug does to the body; deals with
mechanisms of action and drug effects in the body
Drug molecules must exert some chemical influence on
one or more constituents of cells in order to produce a
pharmacological response.
Since drug molecules are few compared to organism
molecules, drugs are not distributed randomly,
otherwise the response would be negligible.
Drugs have to bind to particular constituents of the
cells/tissues to exert their effect. The utility of a drug
pharmacologically is determined by its ability to act on
specific tissues/ cells i.e. drugs show binding site
specificity.
Pharmacodynamics:
3.
To beable to produce therapeutic effects drugs bind on
protein molecule(targets).
The common protein molecules (targets) on which
drugs bind include.
i. Enzymes
ii. Carrier molecules
iii. Ion channels
iv. Receptors.
4.
An overview ofthe mechanisms of drug action shows that
drug act on:
1. The cell membrane by:
Action on specific receptors e.g agonists and
antagonists on adrenoceptors, histamine receptors,
acetylcholine receptors.
Activation or Inhibition of membrane bound enzymes .
Physiochemical interactions eg general and local
anaesthetics act by disordering the neural membranes,
thereby altering the Na+
influx
Mechanisms of Drug action
5.
2. Metabolic processeswithin the cell by:
E.g most antimicrobial agents act by altering metabolic
processes unique to micro-organisms eg penicillins
interfere with the formation of bacterial cell wall.
3. Outside the cell by:
direct chemical interaction Antacids (bases) interact
with acid in the stomach to produce neutral salts.
Osmosis : Osmotic diuretics (e.g mannitol )are not
reabsorbed by the kidney; create osmotic pressure in
renal tubules, hence loss of water
Laxatives (e.g magnesium sulfate) work in the intestine
by the osmotic pressure principle
6.
Selective toxicityis the principle behind the action of
antimicrobials.
The drugs have to cause alteration of metabolic process of
micro-organisms without affecting the human body .
This is possible because there are exploitable differences
between the micro-organism cell and the human cell.
Such mechanisms of action include:
i. Inhibition of bacterial cell wall synthesis by beta lactam
antibiotics
ii. Inhibition of bacterial ribosome by some antibiotics
iii. Inhibition of ergosterol formation by antifungal agents
iv. Inhibition of micro-organisms’ enzymes
v. Inhibition of bacterial DNA/RNA formation
Mechanism of action of
Antimicrobials
7.
Receptors:
macromolecules involved inchemical signaling between
and within cells;
they may be located on the cell surface membrane or
within the cytoplasm
Ligands
molecules (eg, drugs, hormones, neurotransmitters) that
bind to a receptor
A ligand may activate or inactivate a receptor; activation
may increase or decrease a particular cell function.
• Activated receptors directly or indirectly regulate cellular
biochemical processes
Drug-Receptor Interactions
8.
• Each ligandmay interact with multiple receptor
subtypes.
• Few if any drugs are absolutely specific for one receptor
or subtype, but most have relative selectivity.
Selectivity is the degree to which a drug acts on a given
site relative to other sites;
–selectivity relates largely to physicochemical binding
of the drug to cellular receptors.
–Selectivity determines the separation between desired
and undesired effects of a drug.
–In an ideal case, if a drug is completely specific, an
effective dose should not elicit any undesired effect.
9.
Affinity: probability ofa drug occupying a receptor at
any given instant
–Affinity determines a drug's ability to affect a given
receptor
Intrinsic activity —degree to which a ligand
activates receptors and leads to cellular response.
• A drug's affinity and activity are determined by its
chemical structure.
10.
• Receptor upregulation and down regulation
–Up regulation: increase in the number and binding
affinity of receptors
–Down regulation: decrease in the number and
binding affinity of receptors.
–Drugs, aging, genetic mutations, and disorders can
increase (up-regulate) or decrease (down-regulate)
the number and binding affinity of receptors.
11.
Agonists and antagonists:
Agonist:a drug which binds to its "receptor" and
produces its characteristic functional effect.
In other words agonist drugs activate receptors to
produce the desired response.
◦ A drug may be a full agonist or partial agonist,
depending on the maximal effect it produces.
◦ Many hormones, neurotransmitters (eg,
acetylcholine, histamine, norepinephrine), and
drugs (eg, morphine , phenylephrine etc ) act as
agonists.
12.
Antagonist: a drugwhich binds to the receptor without
causing an effect, thereby preventing an active
substance from gaining access.
• Antagonists prevent receptor activation.
• Preventing activation has many effects.
–increase in cellular function if they block the action
of a substance that normally decreases cellular
function.
–decrease in cellular function if they block the action
of a substance that normally increases cellular
function.
13.
Antagonists maybe of various types:
◦ Reversible antagonists readily dissociate from
their receptor;
◦ Irreversible antagonists form a stable, permanent
or nearly permanent chemical bond with their
receptor (eg, ones forming covalent bonds).
◦ Pseudo-irreversible antagonists slowly dissociate
from their receptor.
14.
Dose-Response Relationships
Adose–response curve is a simple X–Y graph
relating the amount of a drug (dose) to the response
Regardless of how a drug effect occurs—through
binding or chemical interaction—the concentration of
the drug at the site of action controls the effect.
◦ However, response to concentration may be
complex and is often nonlinear.
15.
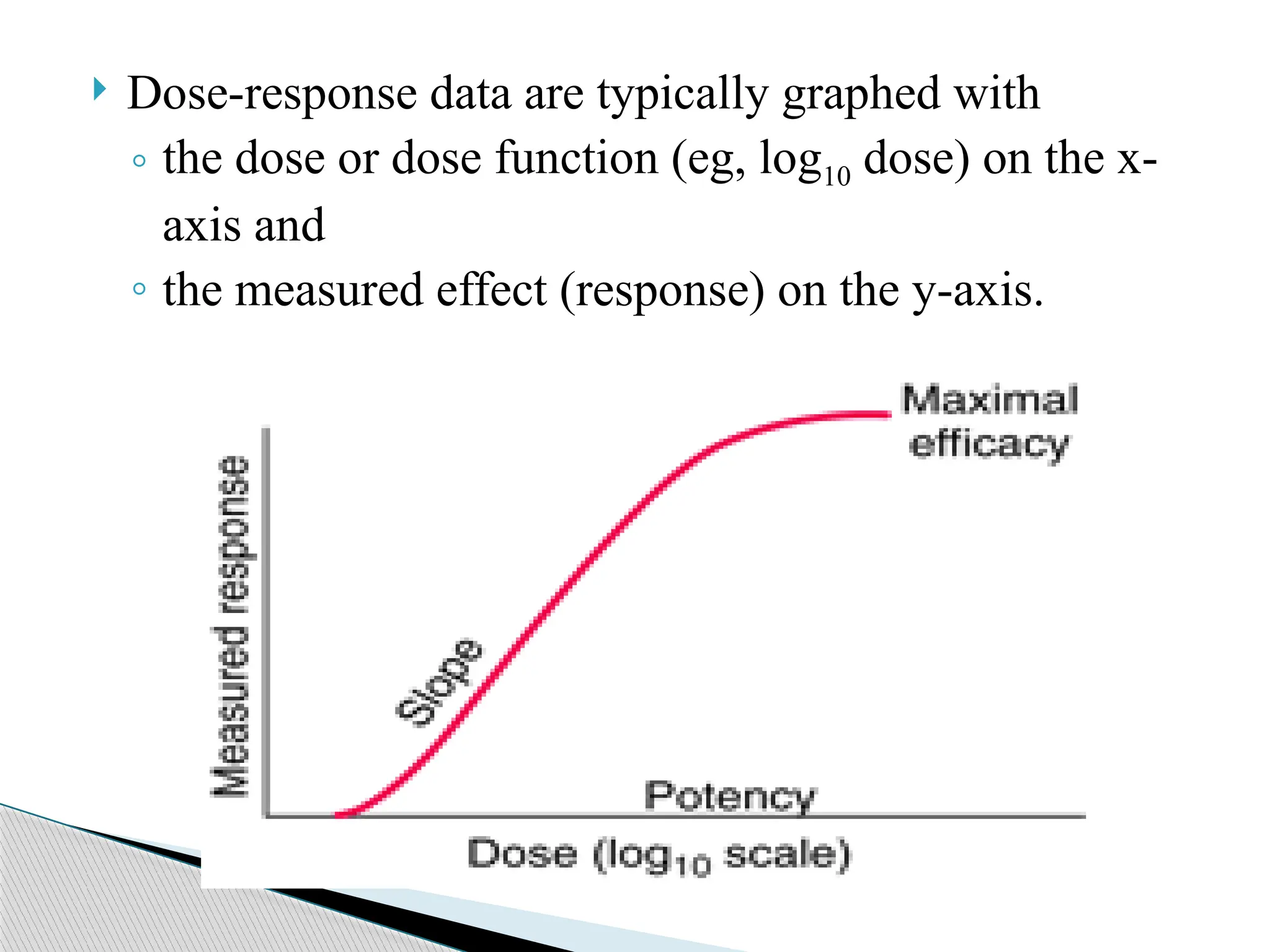
Dose-response dataare typically graphed with
◦ the dose or dose function (eg, log10 dose) on the x-
axis and
◦ the measured effect (response) on the y-axis.
16.
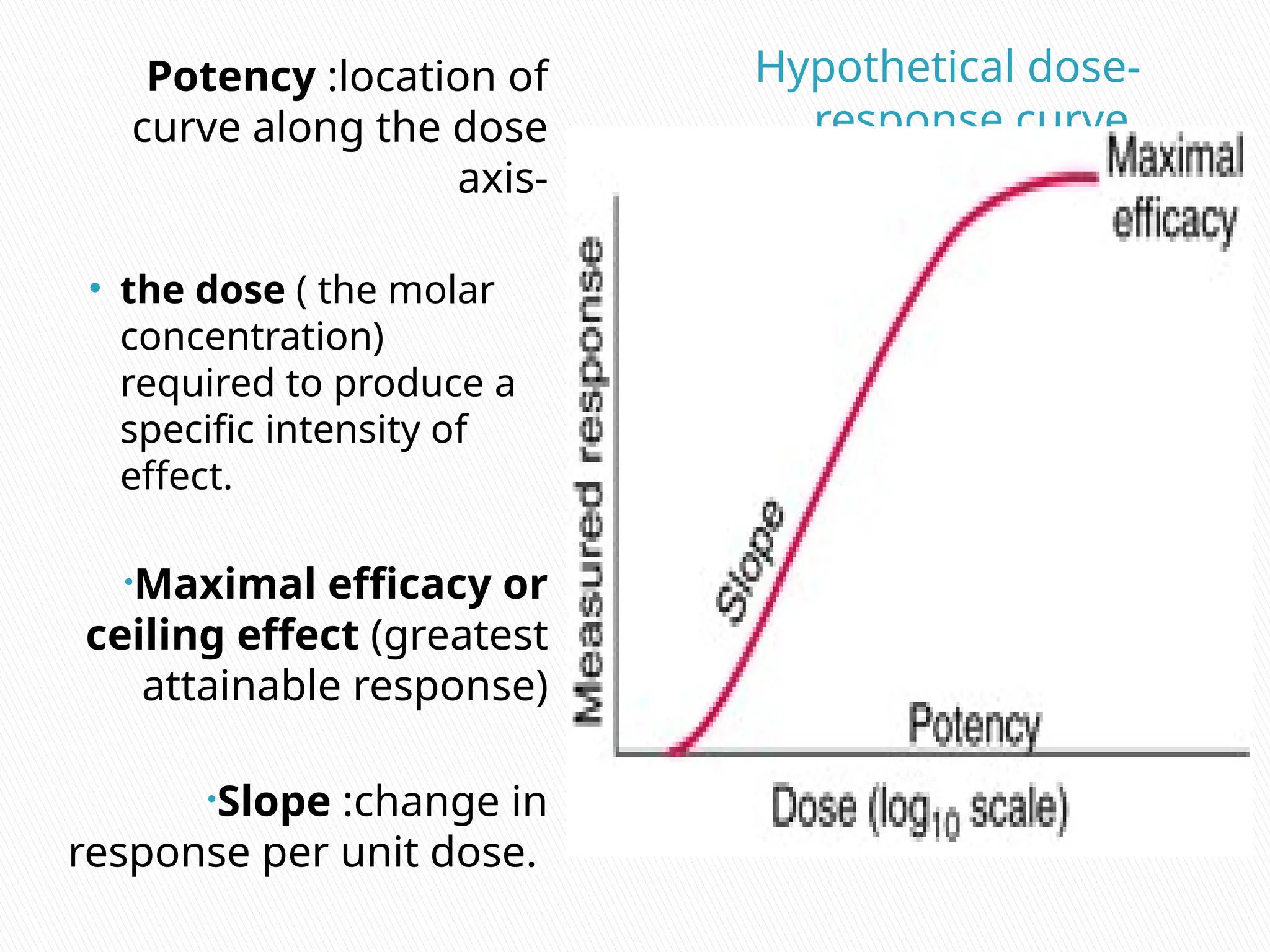
Hypothetical dose-
response curve.
Potency:location of
curve along the dose
axis-
• the dose ( the molar
concentration)
required to produce a
specific intensity of
effect.
•Maximal efficacy or
ceiling effect (greatest
attainable response)
•Slope :change in
response per unit dose.
17.
Potency: Thepotency of a drug refers to the dose
(actually the molar concentration) required to
produce a specific intensity of effect.
ED50
. The median effective dose, or the dose which
produces a response in 50% of subjects.
Maximal efficacy or ceiling effect (greatest
attainable response)
Slope :change in response per unit dose.
Biologic variation: variation in magnitude of
response among test subjects in the same population
given the same dose of drug.
18.
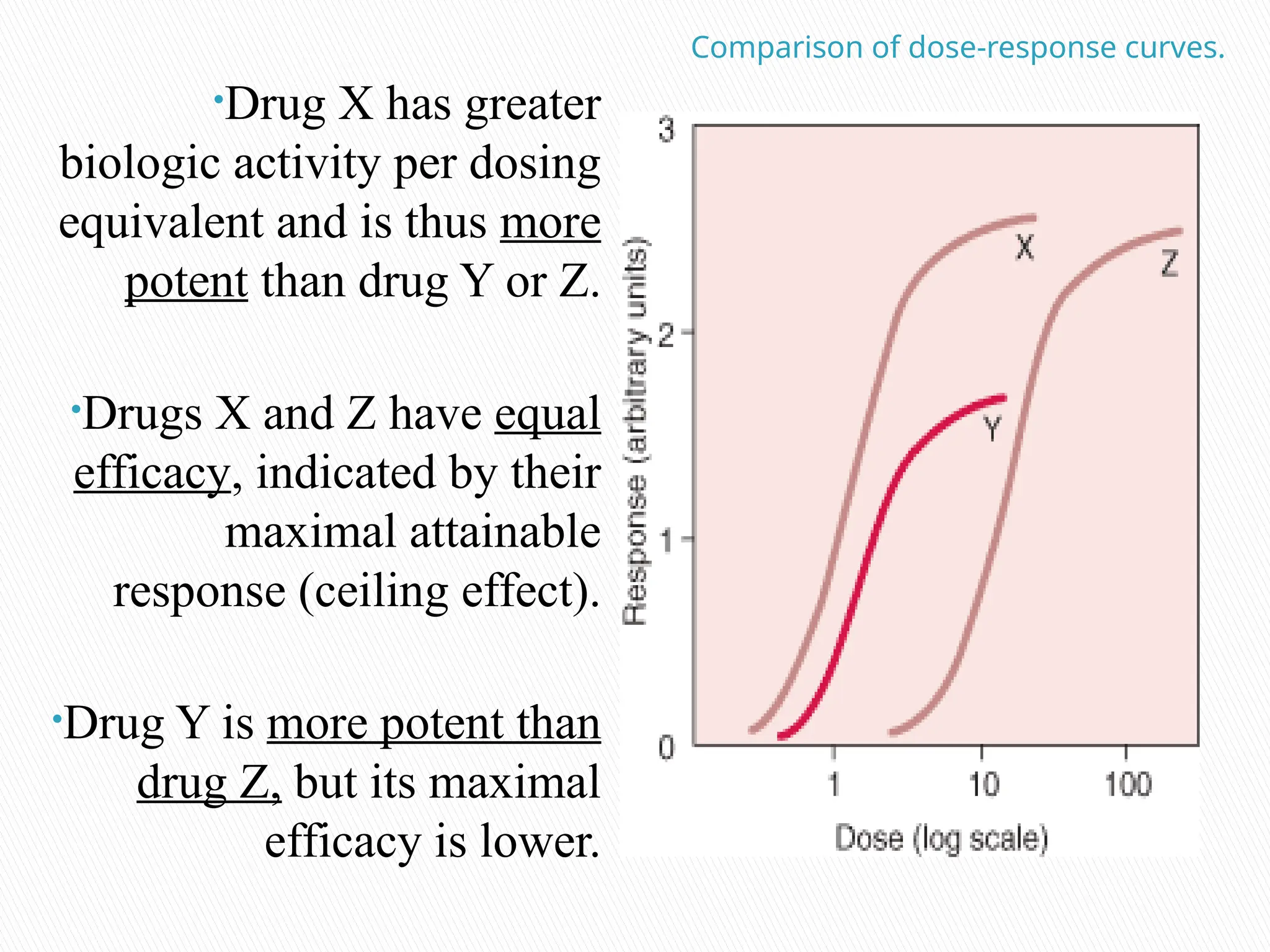
Comparison of dose-responsecurves.
•Drug X has greater
biologic activity per dosing
equivalent and is thus more
potent than drug Y or Z.
•Drugs X and Z have equal
efficacy, indicated by their
maximal attainable
response (ceiling effect).
•Drug Y is more potent than
drug Z, but its maximal
efficacy is lower.
19.
Therapeutic Window.
DEF:The range of dosage of a drug or of its
concentration in the bodily system that provides safe
effective therapy.
◦ For every drug, there exists some concentration
which is just barely effective (the Effective
Concentration) and some dose which is just barely
toxic (the Toxic Concentration).
◦ Between them is the therapeutic window where
most safe and effective treatment will occur.
20.
• A drug'spharmacodynamics can be affected by
physiologic changes due to disorders, aging, or other
drugs.
• Examples of Disorders affecting pharmacodynamic
responses:
–genetic mutations,
–malnutrition,
–some forms of insulin-resistant diabetes mellitus.
• These disorders can change receptor binding, alter the
level of binding proteins, or decrease receptor
sensitivity.
• Aging tends to affect pharmacodynamic responses
through alterations in receptor binding.
Editor's Notes
#3 Digitalis, a drug still used in heart failure, inhibits the activity of the carrier molecule, Na-K-ATPase pump
General anesthetics were once thought to work by disordering the neural membranes, thereby altering the Na+ influx.
aspirin irreversibly inhibits the enzyme prostaglandin synthetase (cyclooxygenase) thereby preventing inflammatory response.
#11 Agonist drugs activate receptors to produce the desired response. Conventional agonists increase the proportion of activated receptors. Inverse agonists stabilize the receptor in its inactive conformation and act similarly to competitive antagonists .
#13 In competitive antagonism, binding of the antagonist to the receptor prevents binding of the agonist to the receptor. In noncompetitive antagonism, agonist and antagonist can be bound simultaneously, but antagonist binding reduces or prevents the action of the agonist. In reversible competitive antagonism, agonist and antagonist form short-lasting bonds with the receptor, and a steady state among agonist, antagonist, and receptor is reached. Such antagonism can be overcome by increasing the concentration of the agonist. For example, naloxone (an opioid receptor antagonist that is structurally similar to morphine), when given shortly before or after morphine , blocks morphine ‘s effects. However, competitive antagonism by naloxone can be overcome by giving more morphine .
Structural analogs of agonist molecules frequently have agonist and antagonist properties; such drugs are called partial (low-efficacy) agonists, or agonist-antagonists. For example, pentazocine activates opioid receptors but blocks their activation by other opioids. Thus, pentazocine provides opioid effects but blunts the effects of another opioid if the opioid is given while pentazocine is still bound. A drug that acts as a partial agonist in one tissue may act as a full agonist in another.
#15 Because a drug effect is a function of dose and time, such a graph depicts the dose-response relationship independent of time. Measured effects are frequently recorded as maxima at time of peak effect or under steady-state conditions (eg, during continuous IV infusion). Drug effects may be quantified at the level of molecule, cell, tissue, organ, organ system, or organism.
#16 Potency :location of curve along the dose axis
Maximal efficacy or ceiling effect (greatest attainable response), and
Slope :change in response per unit dose.
Biologic variation: variation in magnitude of response among test subjects in the same population given the same dose of drug.
#20 Pharmacodynamic drug–drug interactions result in competition for receptor binding sites or alter postreceptor response.
![PRINCIPLES OF PHARMOCODYNAMICS 2 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/principlesofpharmocodynamics2autosaved-230607181037-758ddb07-thumbnail.jpg?width=640&height=640&fit=bounds)


































































