Download to read offline

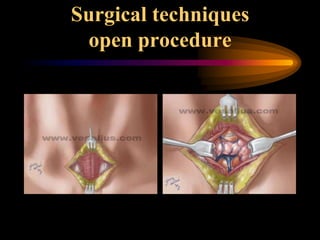
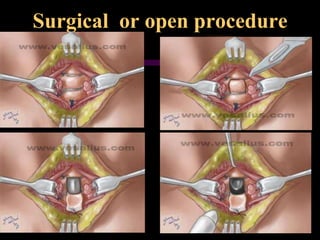
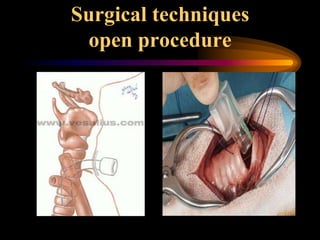





1. The document compares the surgical and percutaneous dilational tracheostomy (PCDT) procedures for creating a tracheostomy from 2013-2015. 2. 51 total cases were performed, with 2 patients requiring conversion to an open procedure due to bleeding complications with PCDT. 3. PCDT was found to be a safe and effective alternative to the open surgical procedure with comparable late complications but lower early bleeding risks and cost.




























![PERCUTANEOUS TRACHEOSTOMY- -NOV[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/percutaneoustracheostomy-dr-240730031420-3891a762-thumbnail.jpg?width=640&height=640&fit=bounds)




















































