Download to read offline




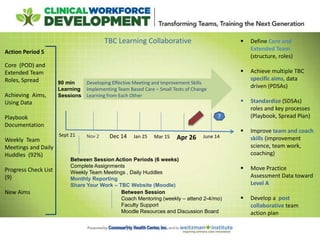








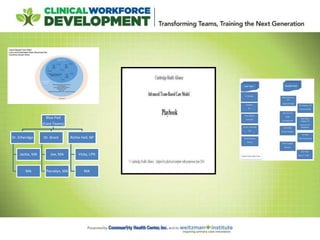












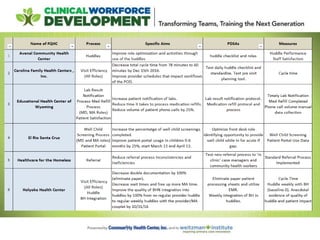
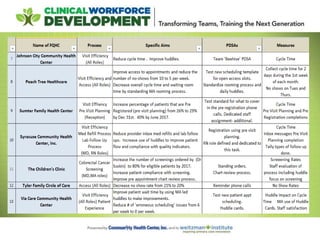

Here are some questions teams have about core and extended teams, pre-visit planning/huddles, self-management goal setting workflows, and the coaching role: Core and Extended Teams: - How are you identifying your patient care teams (PODS) so staff and patients know their team? - What specific roles have you seen change on teams and how? - How are you training staff on team-based care? - How do you maintain team integrity with turnover/MAs covering multiple teams? - Are managers/leaders part of your core and extended team model? Pre-Visit Planning and Huddles: - How do you manage prep time for huddles? Are