



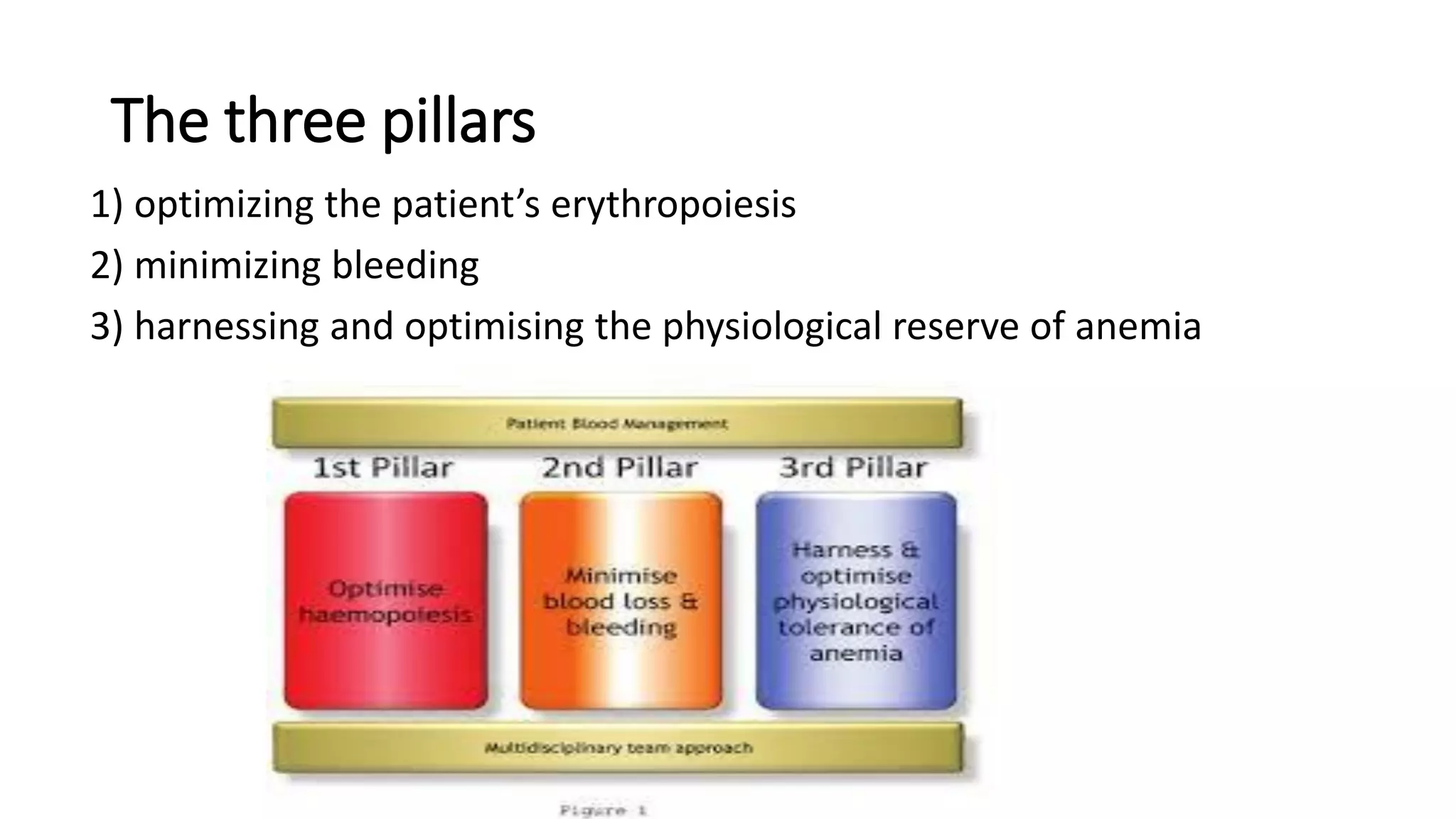




















This document discusses patient blood management (PBM), which is a multidisciplinary approach to optimizing patient care and reducing unnecessary blood transfusions. It has three pillars: optimizing erythropoiesis, minimizing bleeding, and harnessing physiological reserves of anemia. The evidence shows PBM can reduce transfusions by 39% without increasing risks. It has led to reduced transfusions and costs in various settings like cardiac and orthopedic surgery. PBM programs require a multidisciplinary team approach led by specialties like anesthesiology. Overall, PBM provides better patient outcomes while reducing allogeneic blood use.



































































