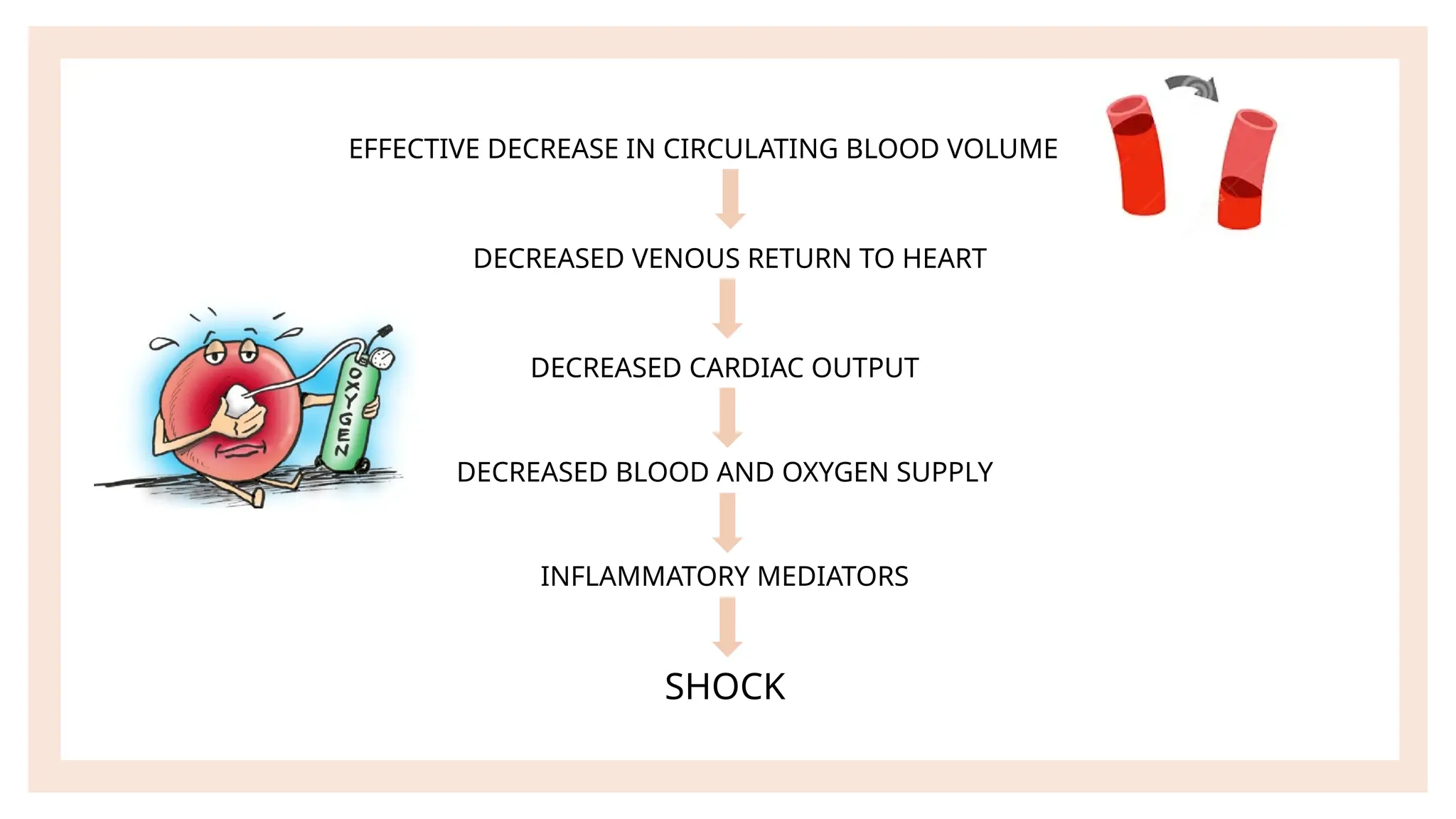
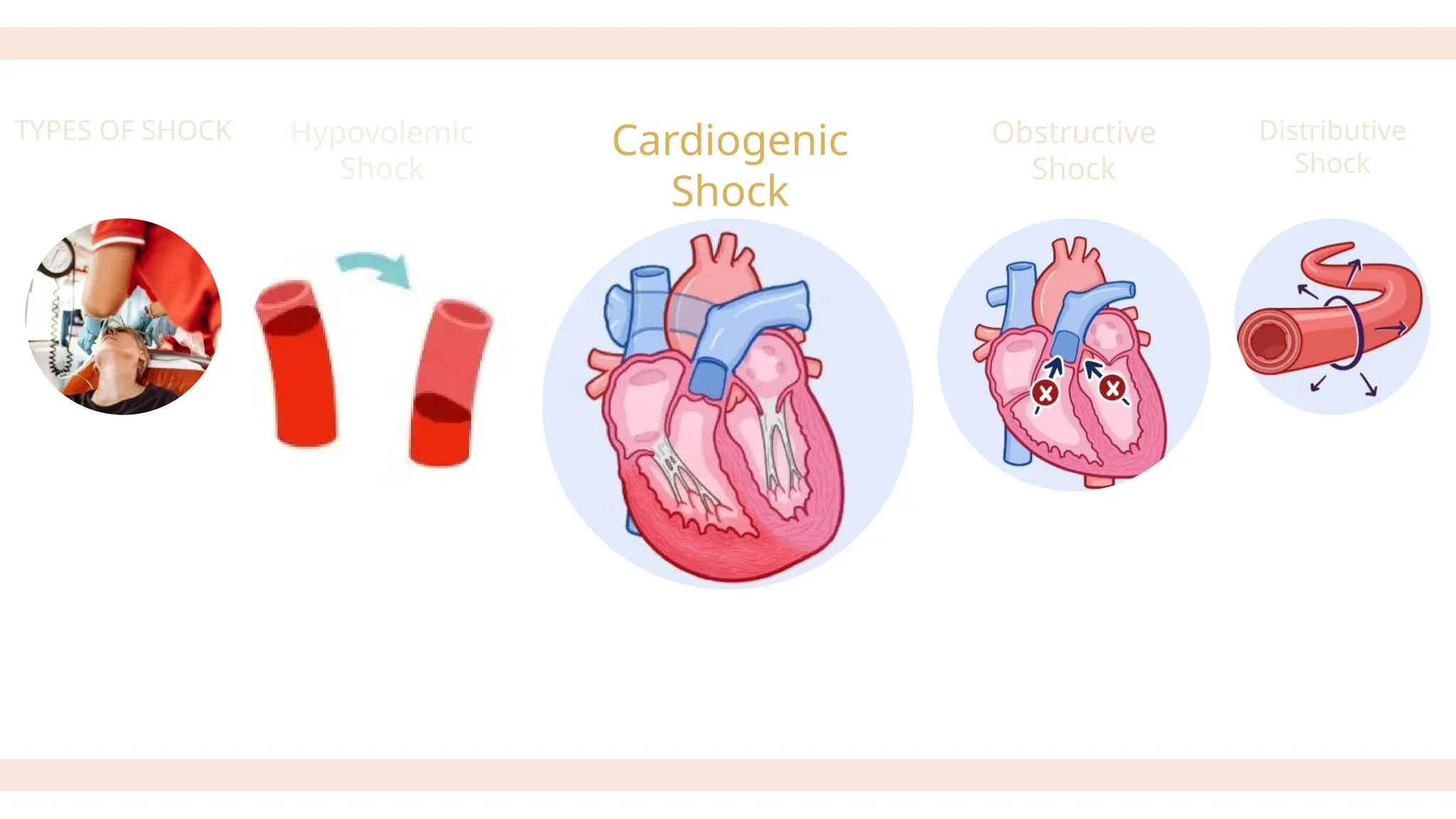
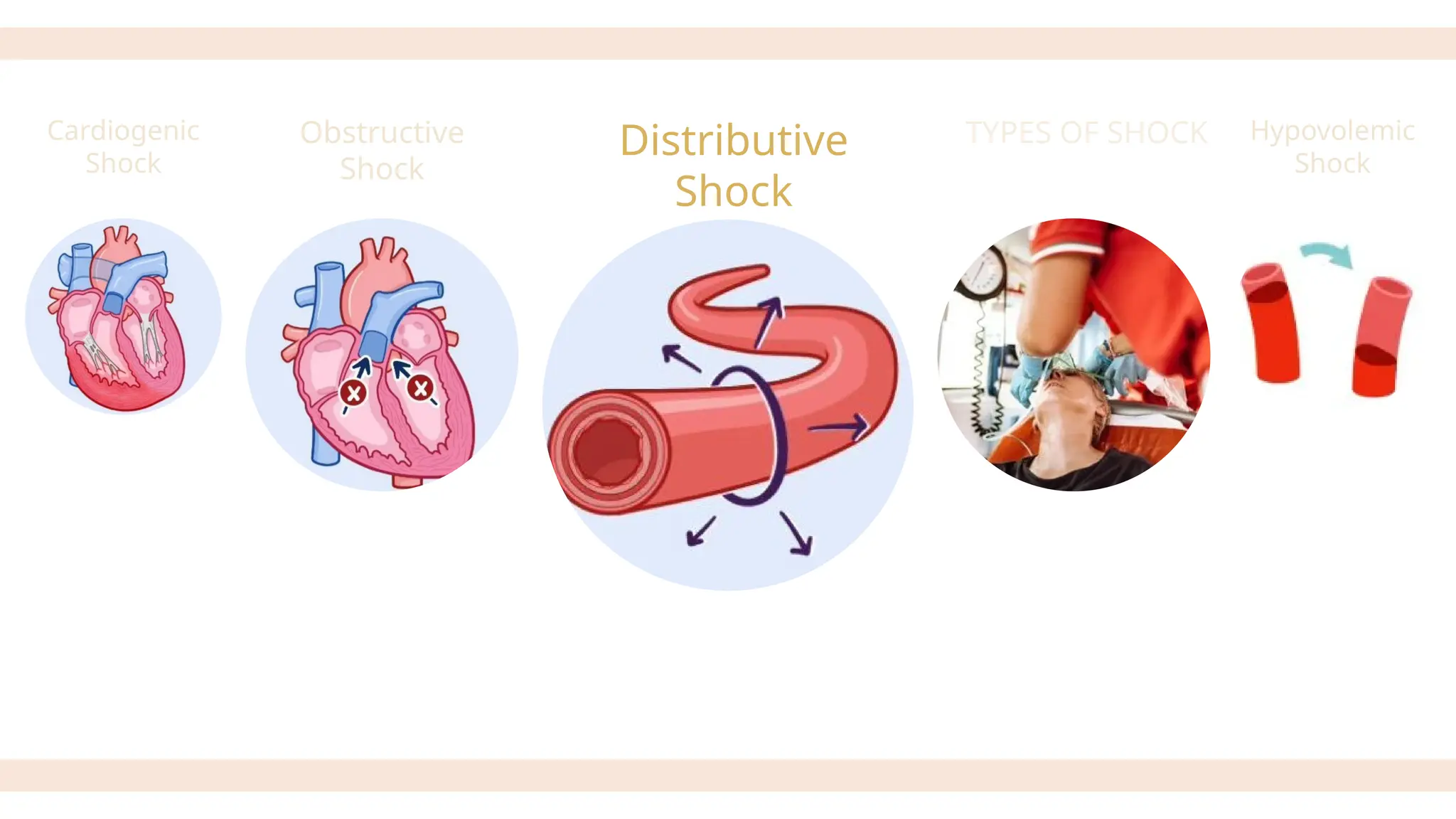
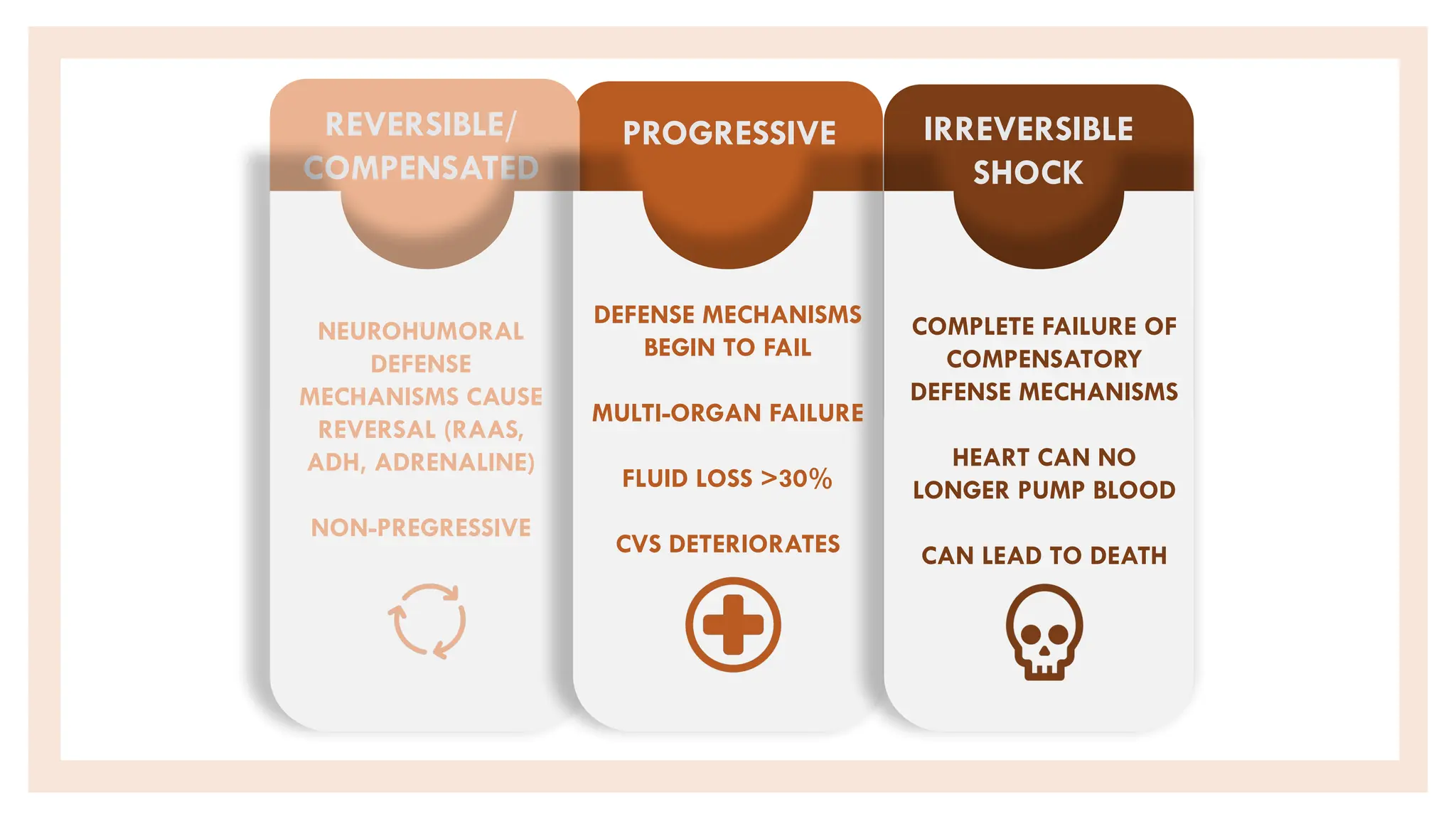
Shock is a critical condition characterized by acute circulatory failure leading to inadequate tissue perfusion and cellular hypoxia, which can result from various causes such as trauma, blood loss, and severe infections. It is classified into primary and secondary types, with types including hypovolemic, cardiogenic, obstructive, and distributive shock; each having distinct pathophysiological mechanisms and clinical features. Early recognition and prompt treatment are essential for managing shock and preventing severe outcomes, including organ failure and death.