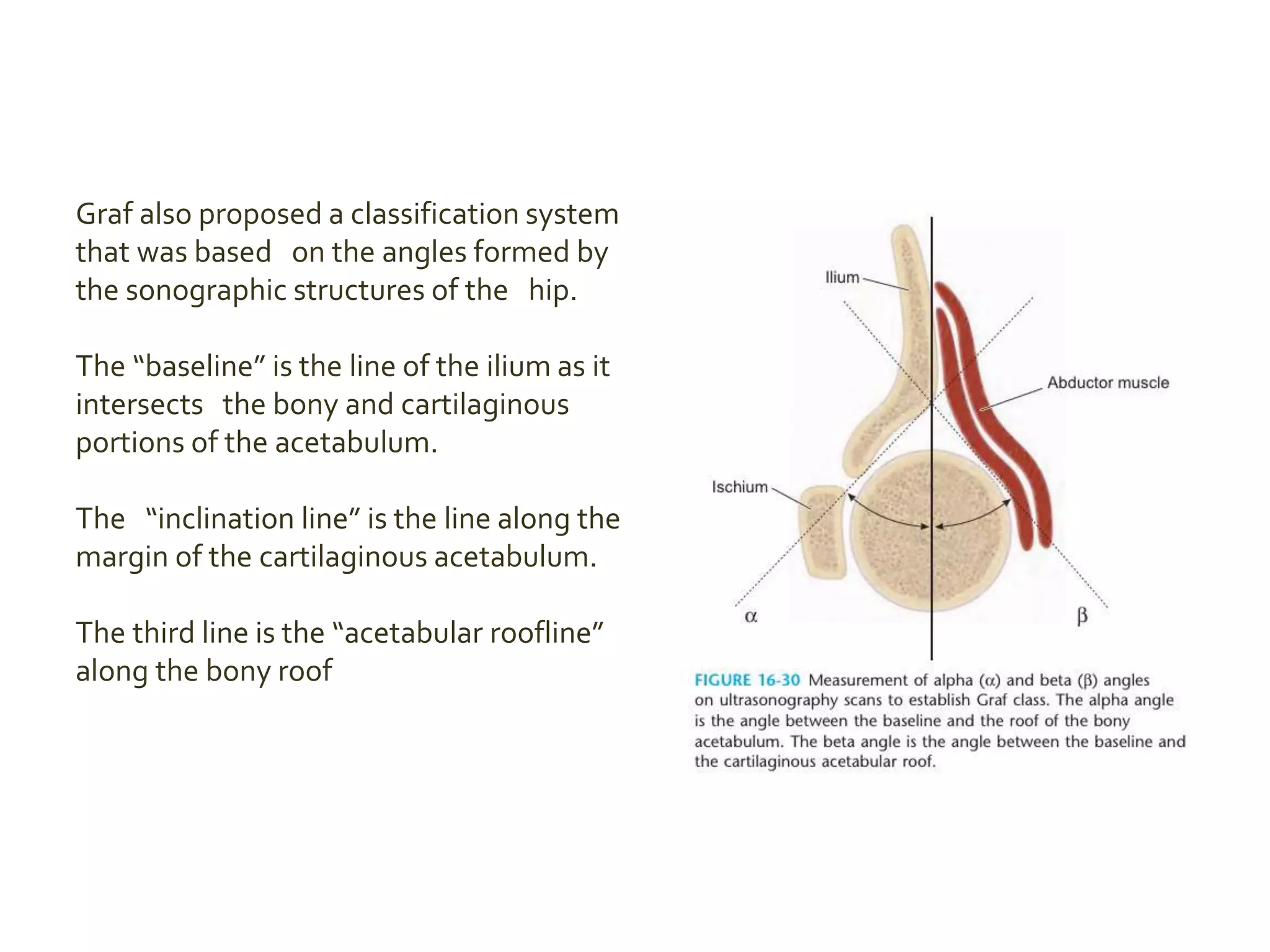
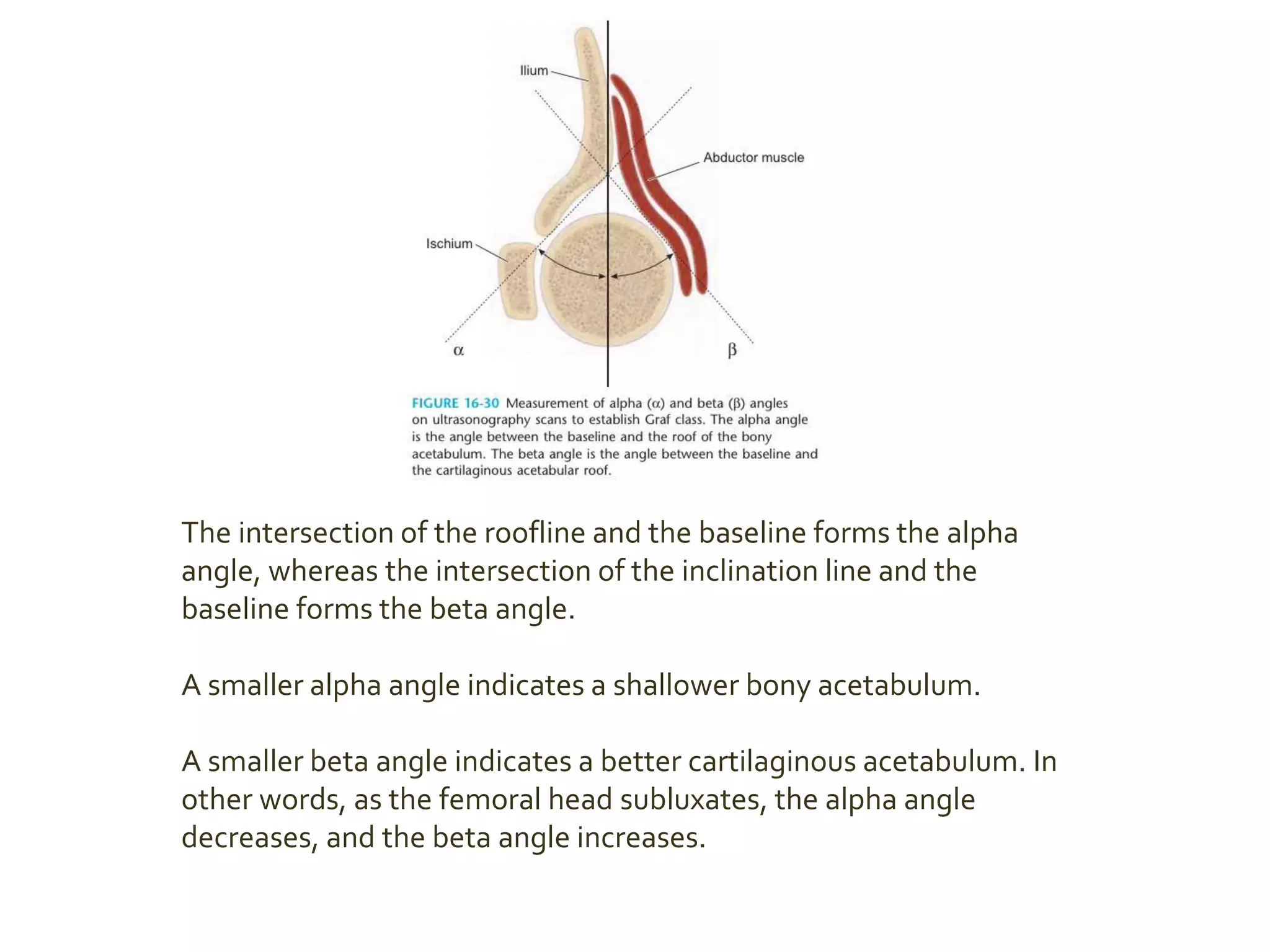
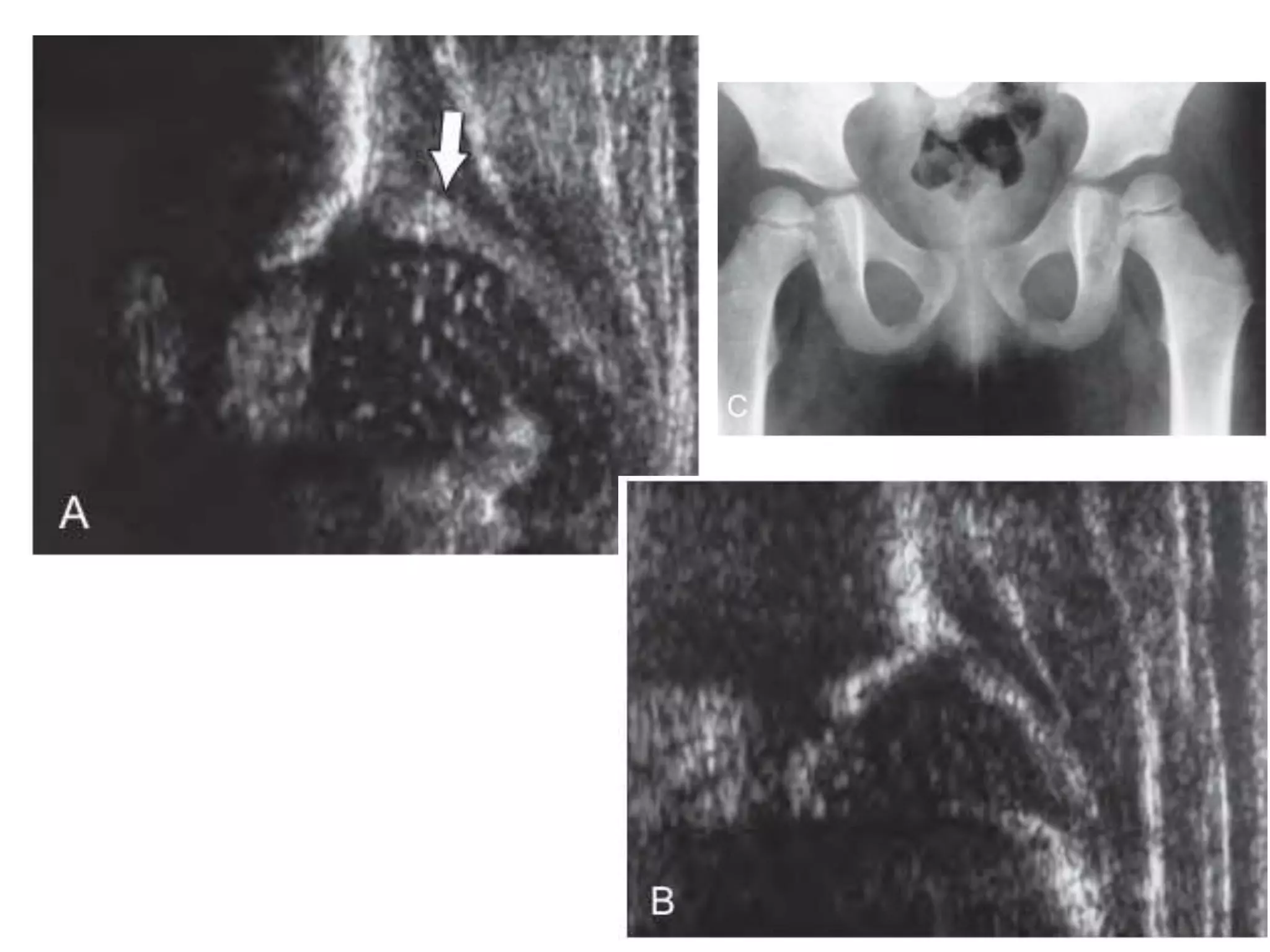
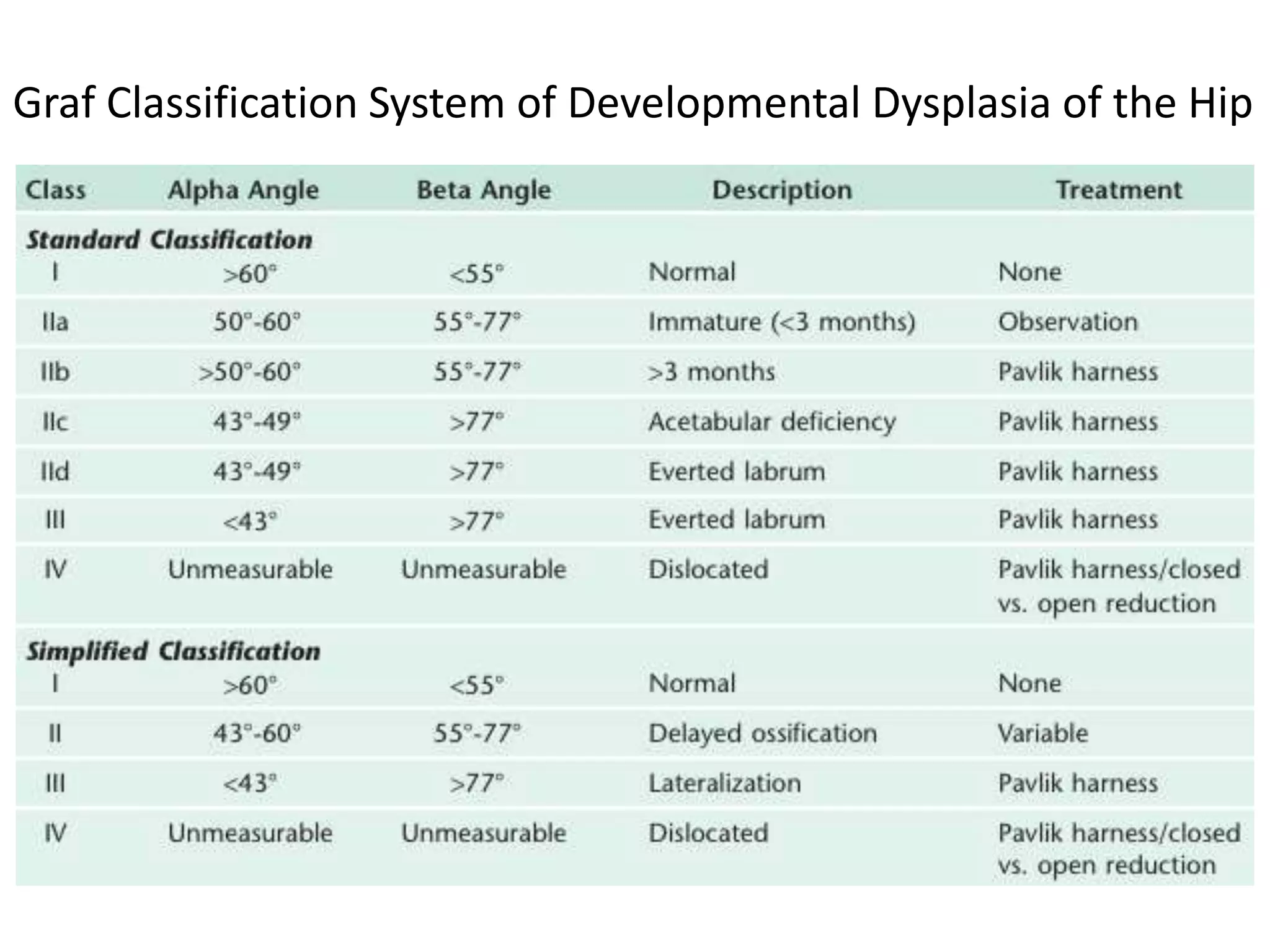
The document discusses the challenges and techniques in diagnosing developmental dysplasia of the hip (DDH) using various radiological methods, especially ultrasonography, which is preferred for its ability to visualize soft tissue anatomy. It highlights the importance of specific angles and classifications in assessing hip stability and identifies concerns about over-treatment due to the sensitivity of sonographic findings. Additionally, it outlines screening criteria for infants at risk of DDH and the limitations of current imaging techniques such as MRI in terms of cost and accessibility.