Downloaded 56 times

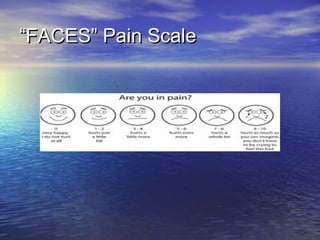



1. EMS providers should receive training in pediatric pain assessment and management to improve care of pediatric patients. Protocols should include pediatric-specific pain management measures. 2. Nonpharmacological strategies like involving child life specialists can help reduce pediatric pain and anxiety. Family presence during procedures can also help. 3. Pain assessment for pediatric patients should begin in the prehospital setting and continue through emergency department discharge with instructions for home pain management.























































































