Download as PDF, PPTX




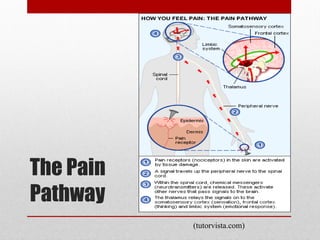
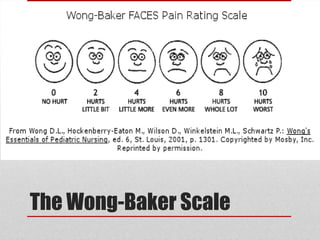
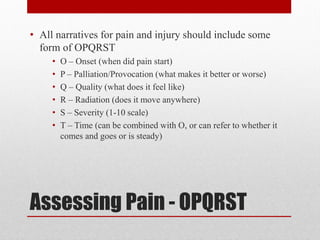







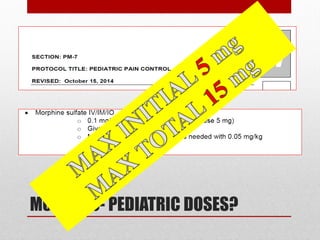
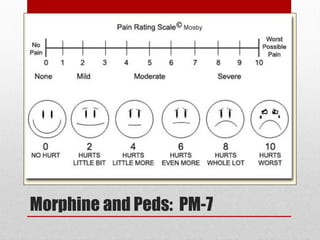
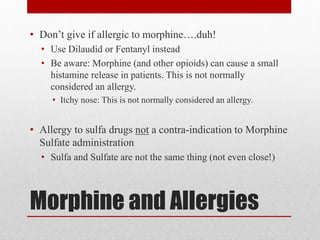
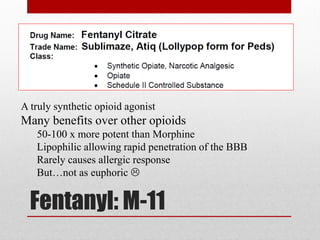
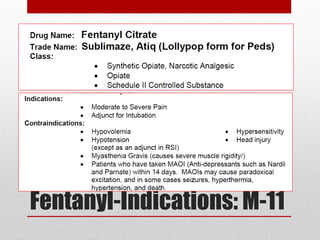
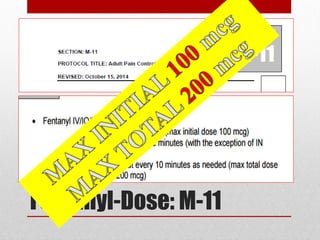
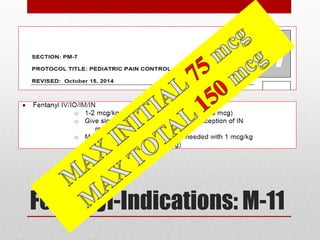
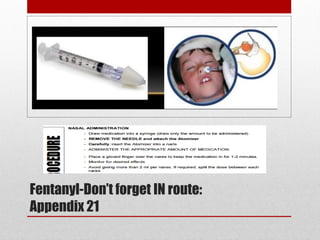









This document provides an overview of pain management for pre-hospital care providers. It defines pain and discusses pain physiology, assessment tools like the numeric pain scale and OPQRST method. It covers types of pain like acute, chronic, referred, somatic and neuropathic. Factors that influence pain tolerance like gender, culture and psychological states are addressed. Guidelines for treating pain to a goal of zero whenever possible are provided, with exceptions for some cases. Non-pharmacological and pharmacological pain management options are outlined.























































































