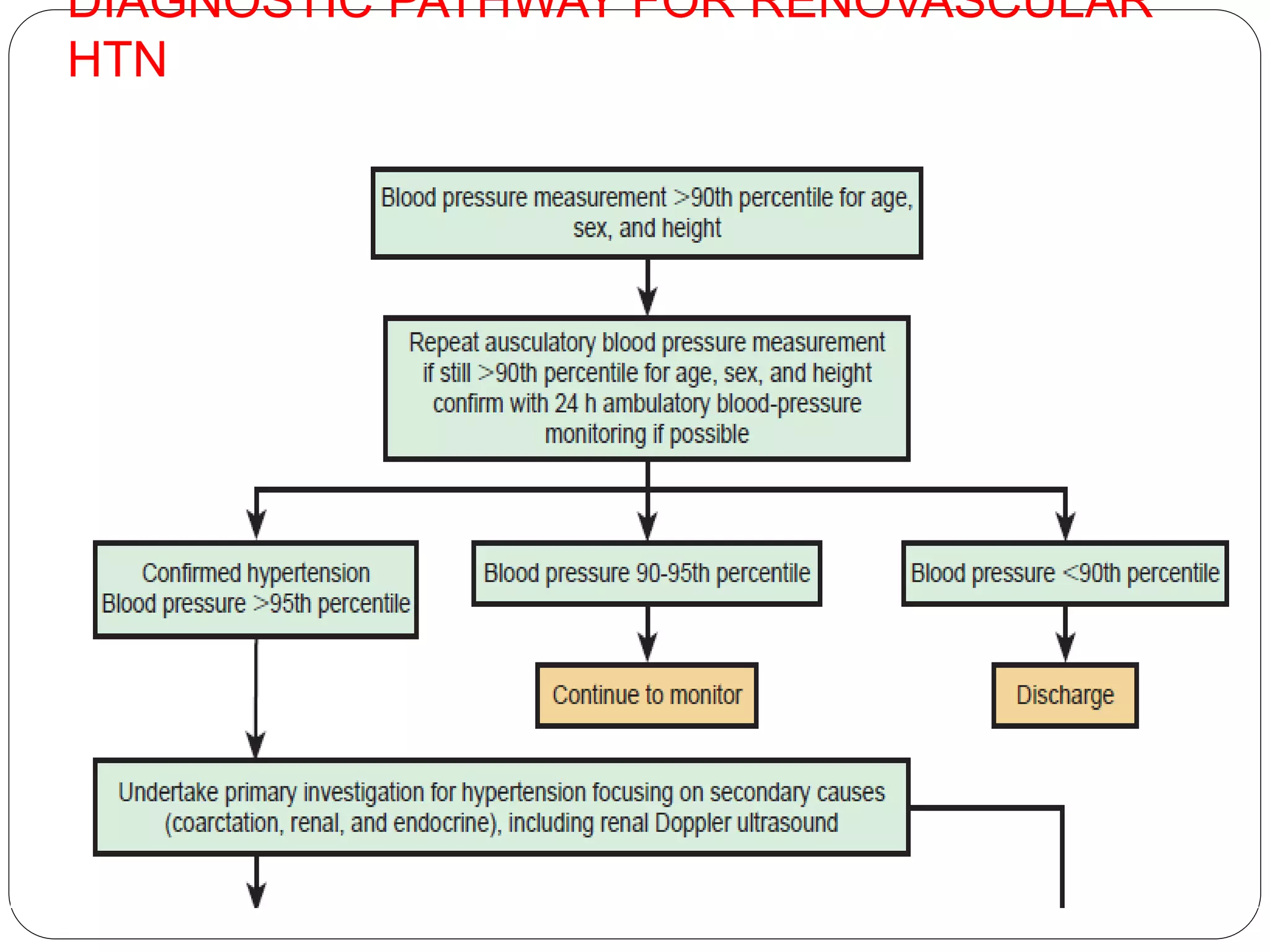
This document summarizes the approach to hypertension in children. It defines hypertension and prehypertension based on blood pressure percentiles for age, gender and height. Secondary causes of hypertension in children include renal, cardiovascular, endocrine and neurological conditions. Evaluation involves assessing for target organ damage and investigating for underlying causes based on clinical features. Treatment involves lifestyle modifications and medications like ACE inhibitors, calcium channel blockers and diuretics based on the patient's age, gender and other health conditions. Hypertensive crisis requires prompt parenteral treatment to lower blood pressure over minutes to hours to prevent complications.