
Downloaded 16 times

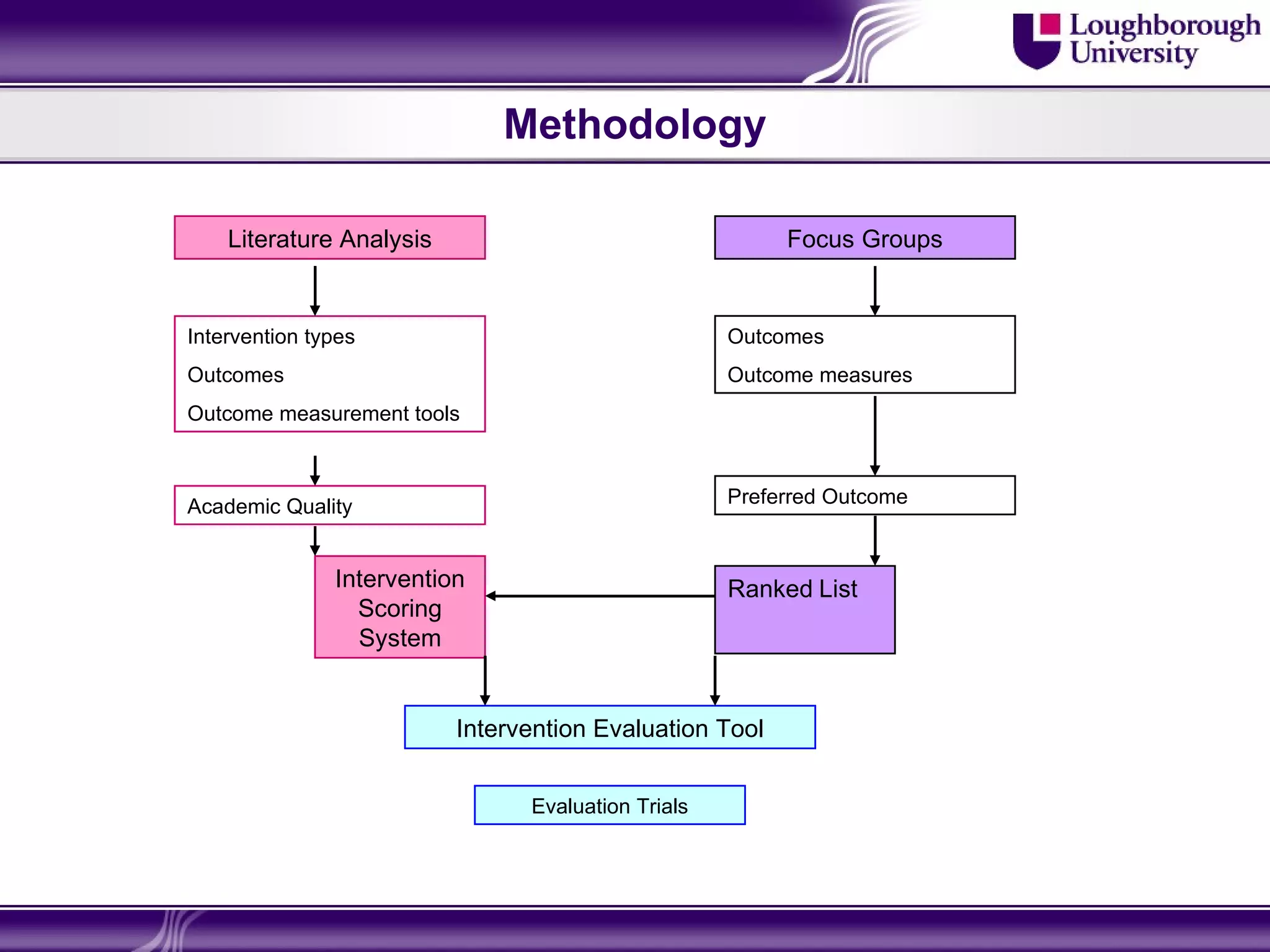
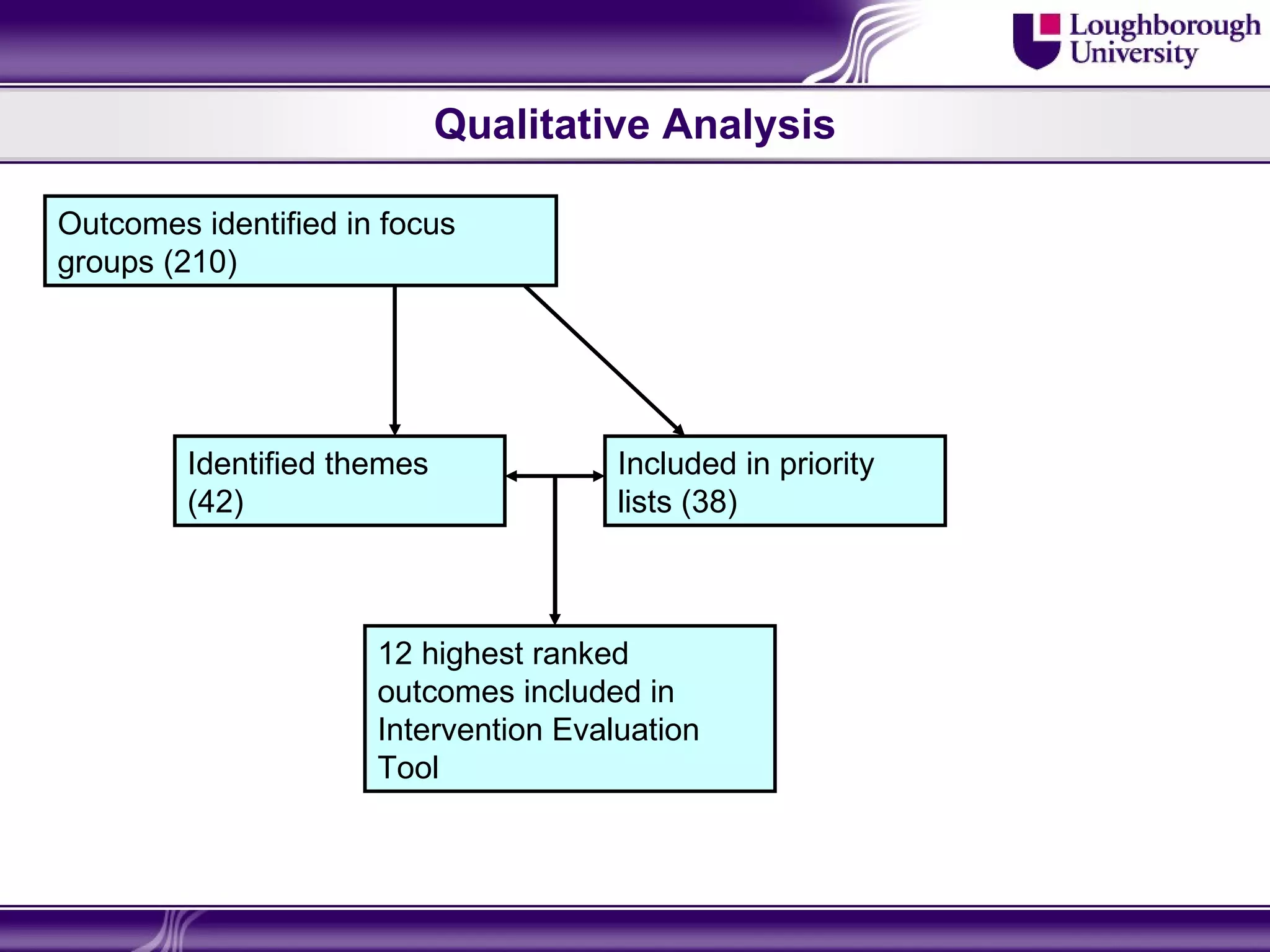
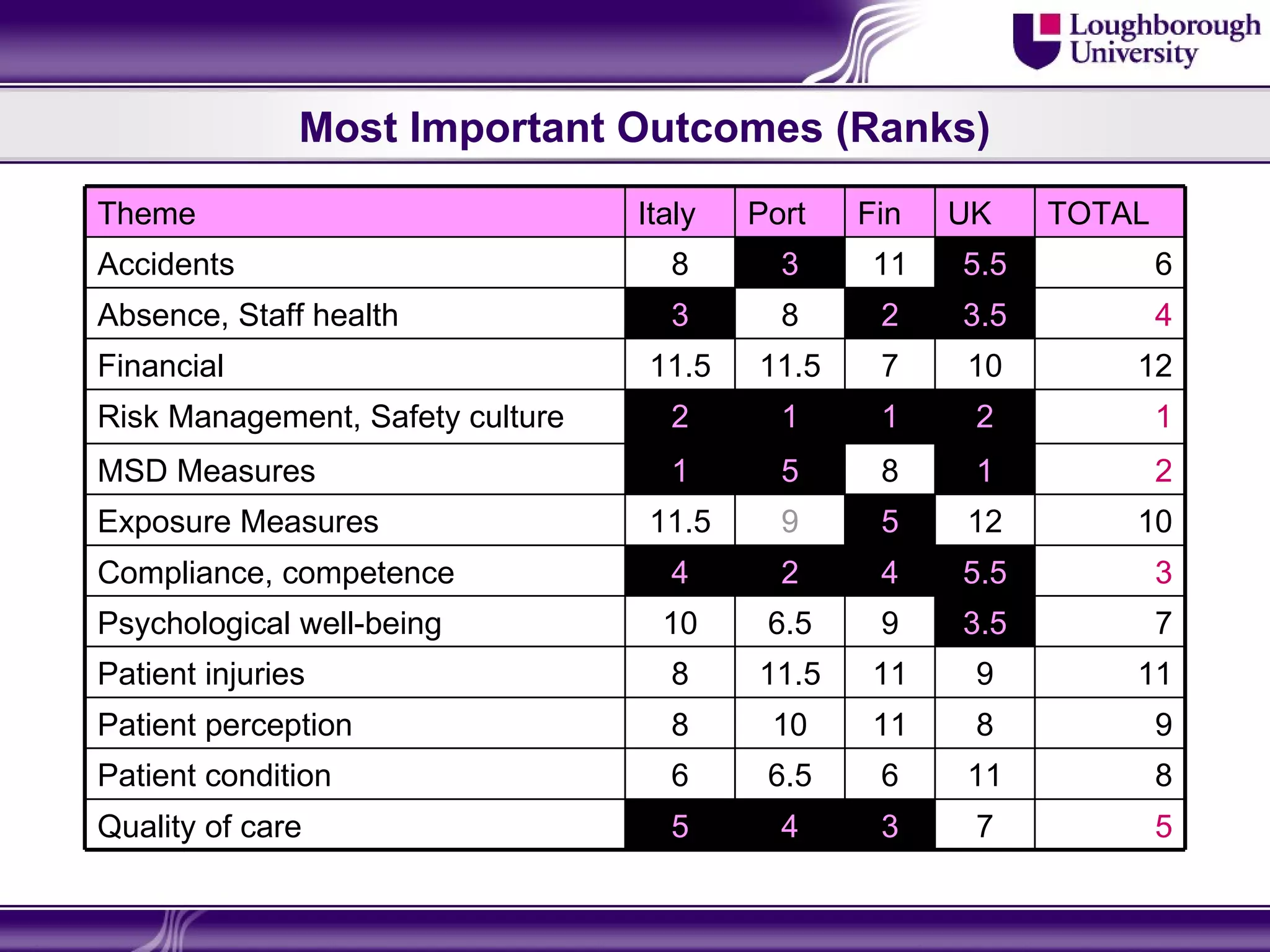
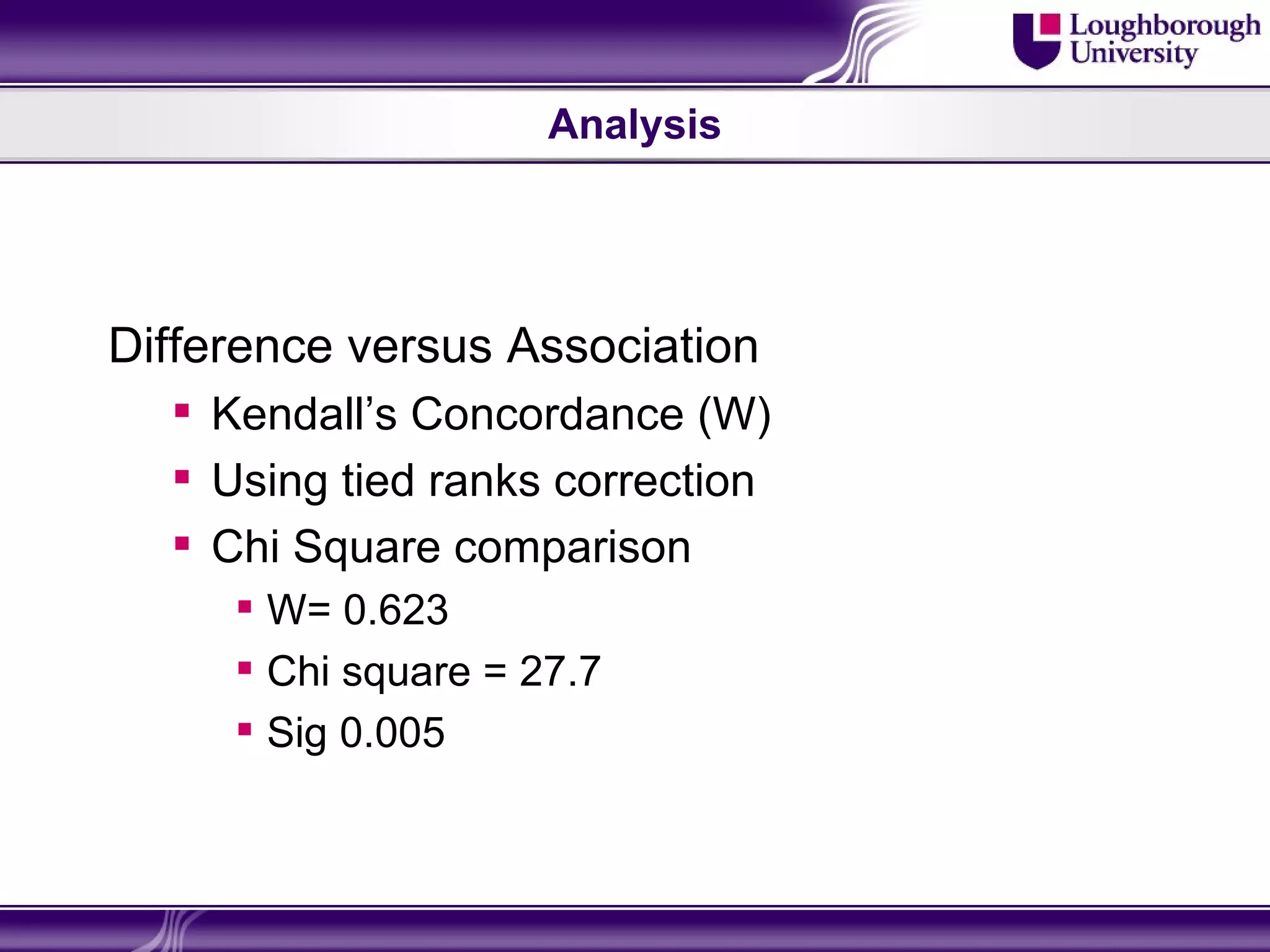
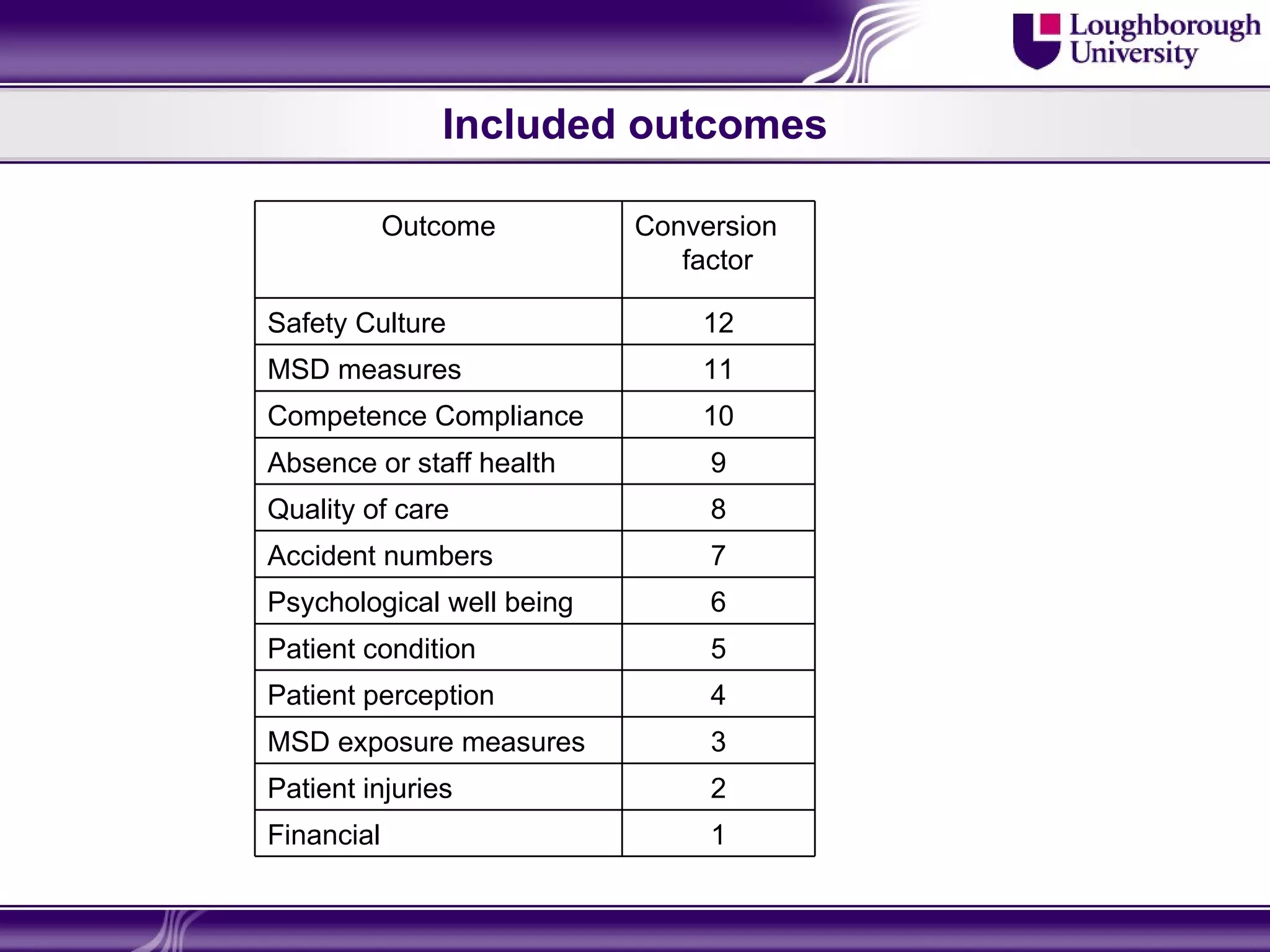
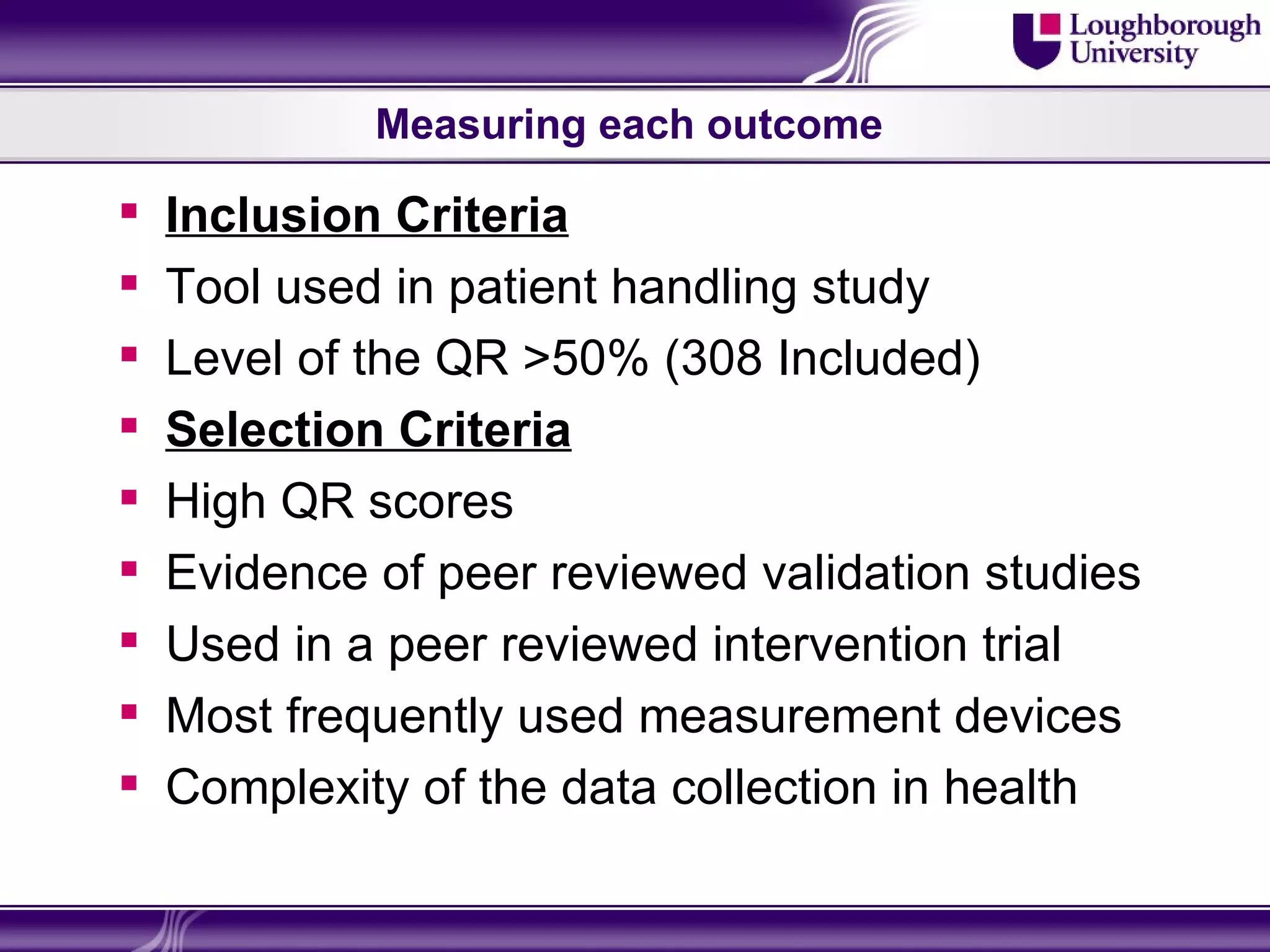
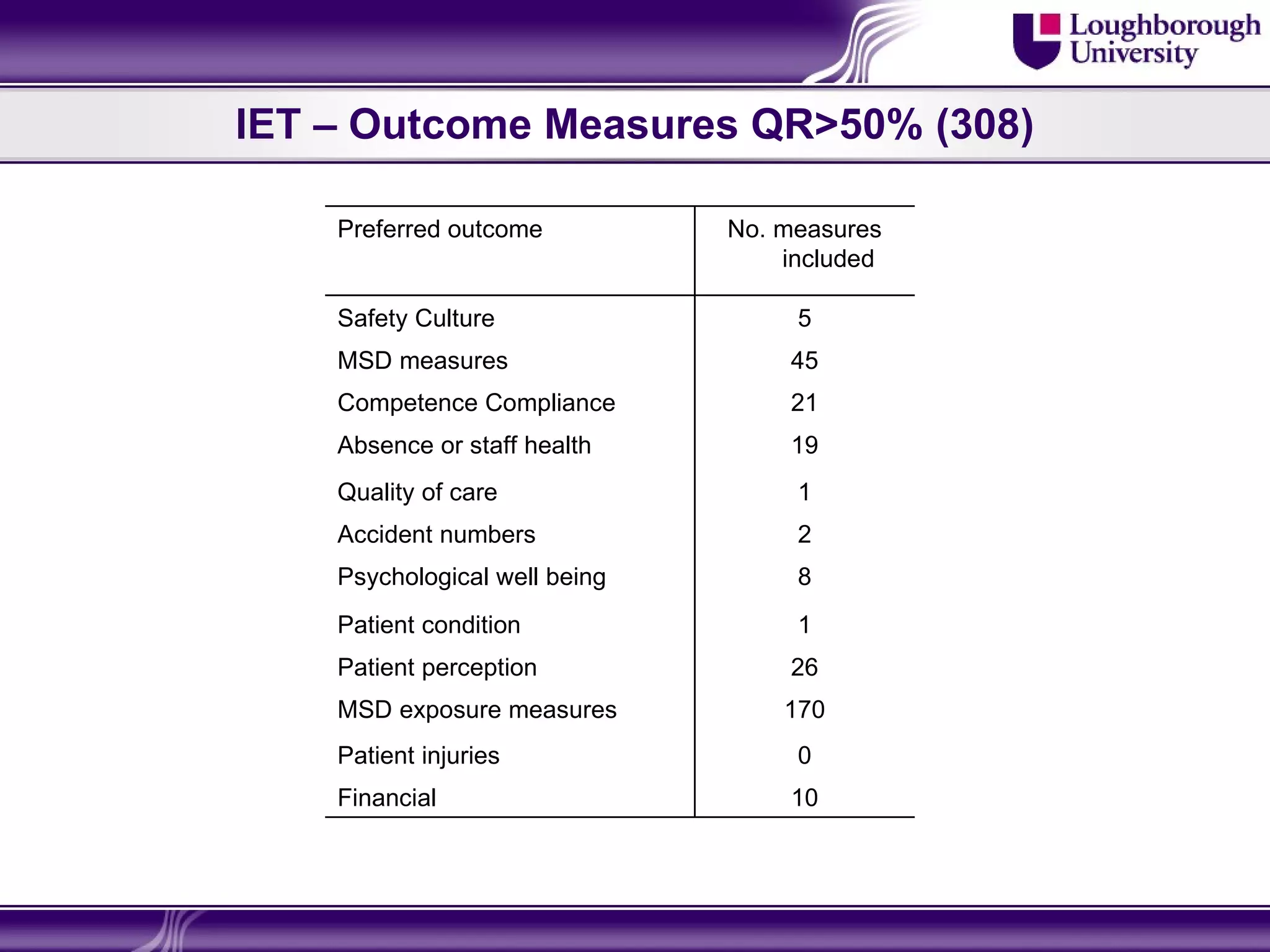
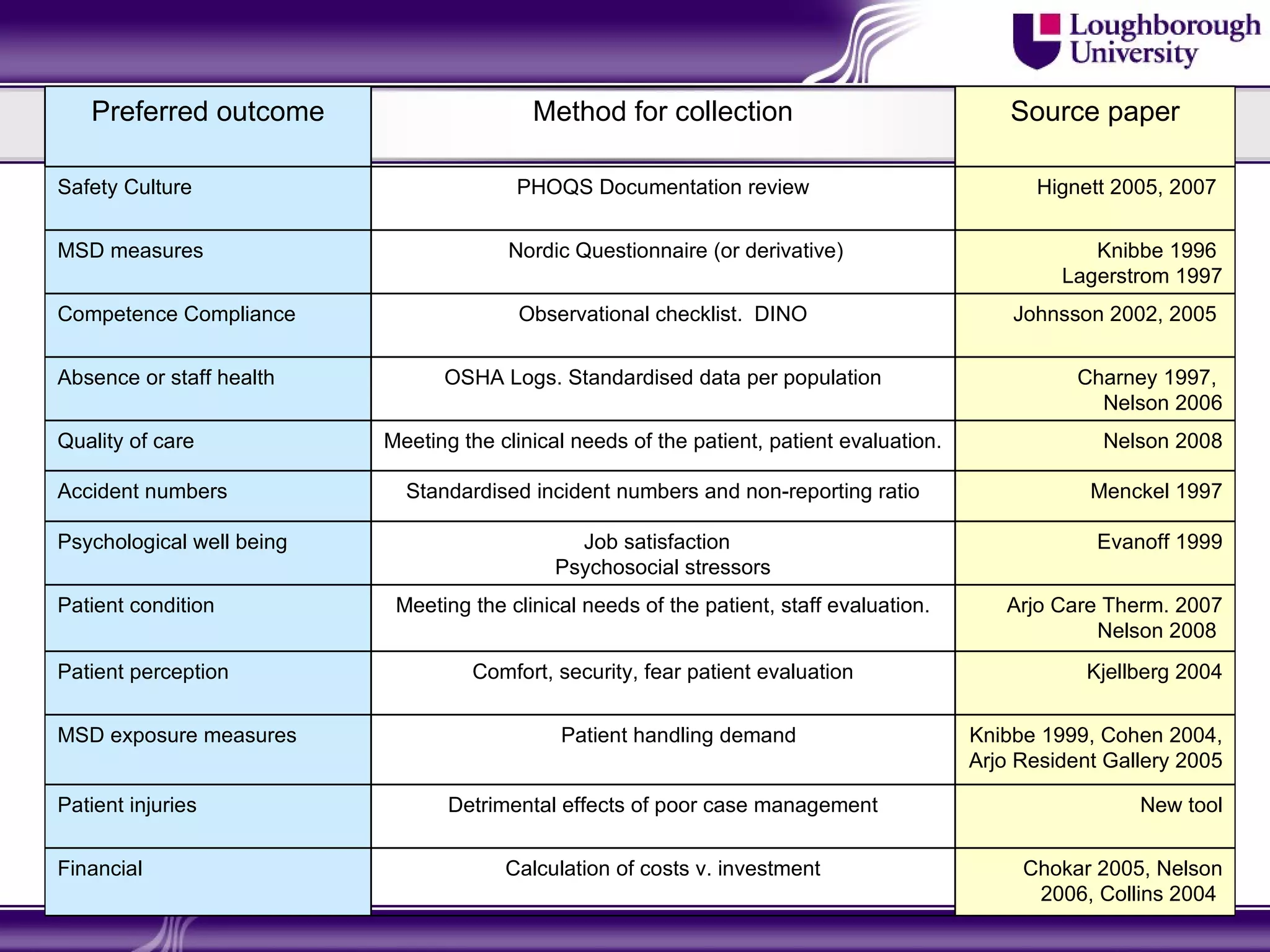

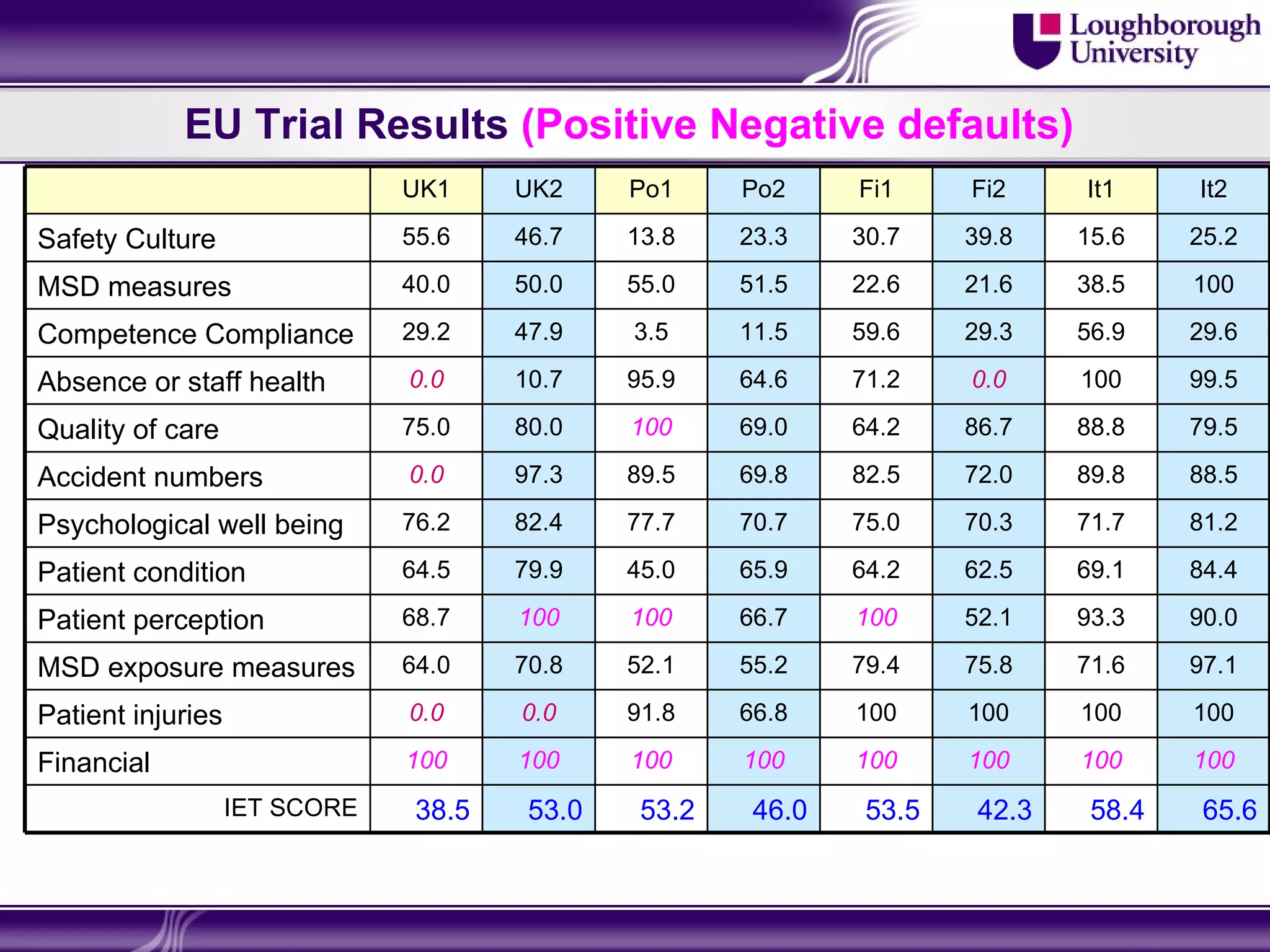
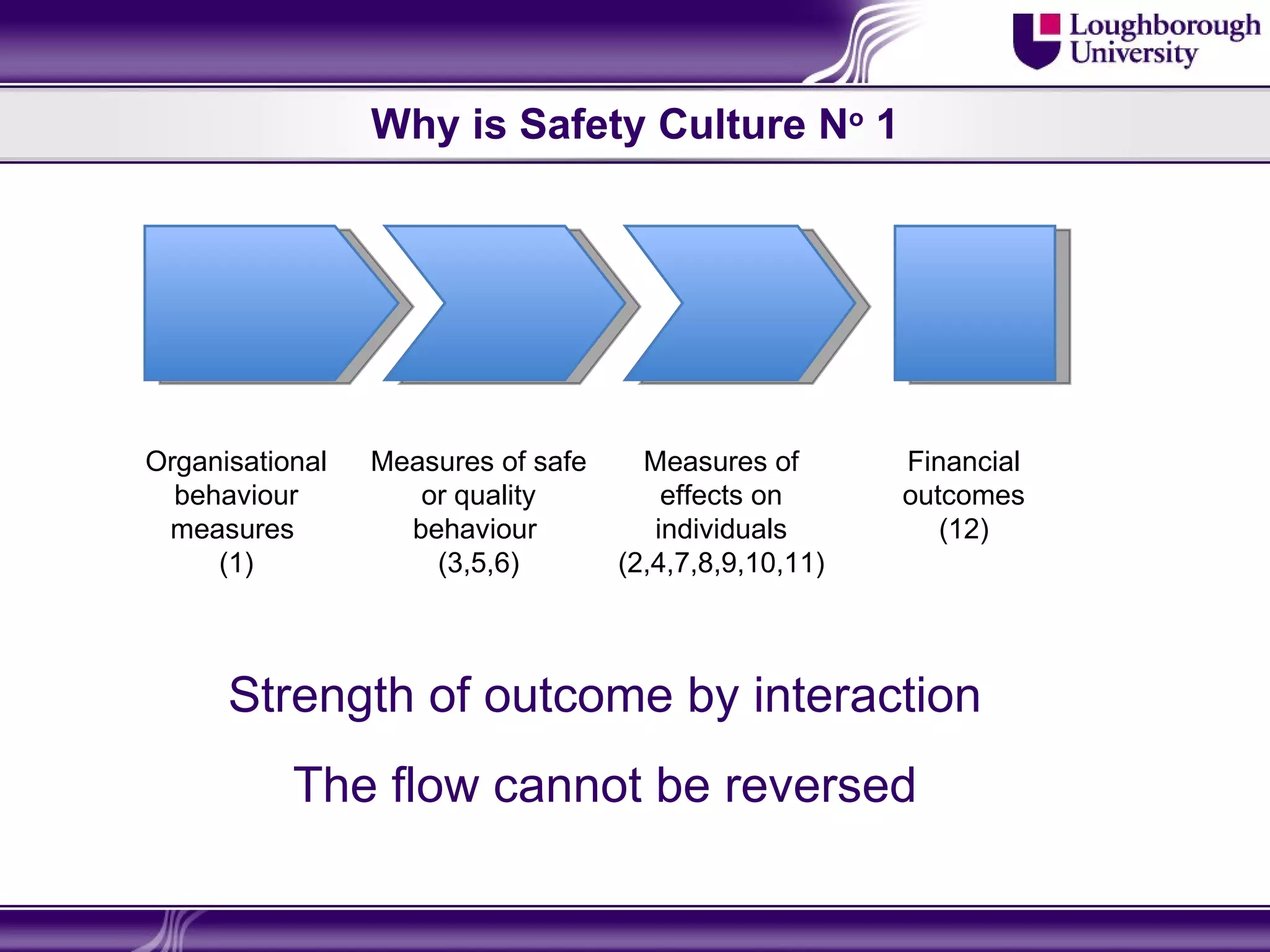

The document discusses the development of a tool to measure the success of patient handling interventions across the EU, addressing the inadequacies of previous reviews that did not adequately identify reductions in musculoskeletal disorders. It outlines the project's methodology, literature analysis, focus group outcomes, and trial results, emphasizing the importance of various outcome measures and the establishment of a standardized evaluation tool. The findings suggest that the tool improves the ability to compare interventions and provides insights for better resource allocation and benchmarking in healthcare settings.






























































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)



