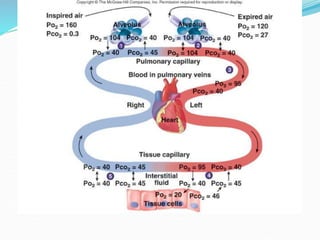
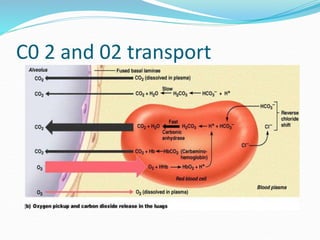
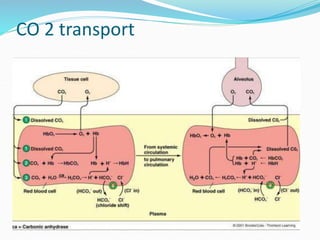
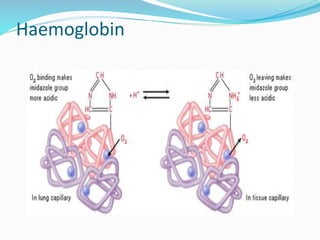
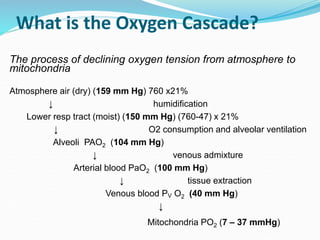
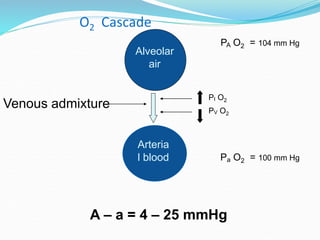
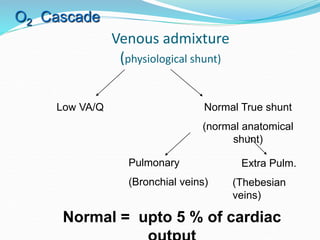
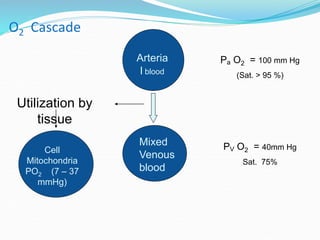
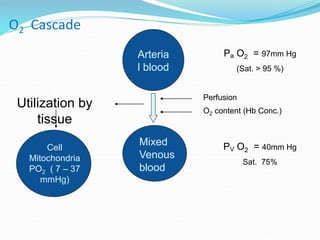
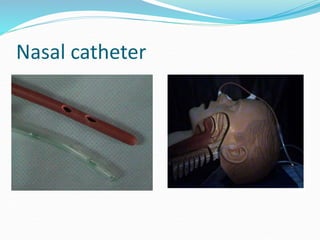
This document provides an overview of oxygen therapy. It discusses oxygen transport and delivery in the body, including how oxygen levels decrease from the atmosphere to tissues. It outlines indications for oxygen therapy when hypoxemia is present. Various oxygen delivery devices are described, including nasal cannulas, masks, and catheters. Low-flow systems provide variable oxygen concentrations while high-flow systems and reservoir masks provide more consistent fixed concentrations. Complications of oxygen therapy are also mentioned.


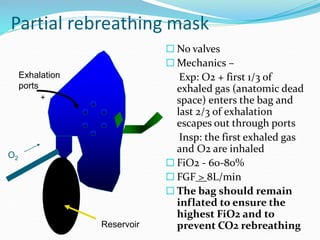
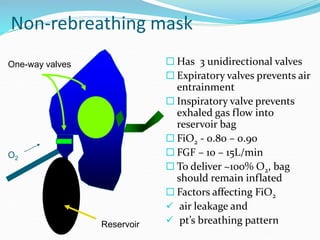







![Mechanical ventilation[1]](https://cdn.slidesharecdn.com/ss_thumbnails/mechanicalventilation1-150109002450-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)





























































