Downloaded 162 times














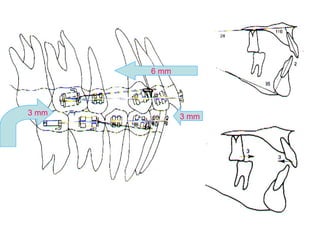
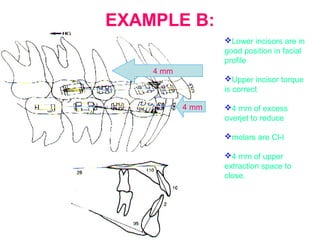
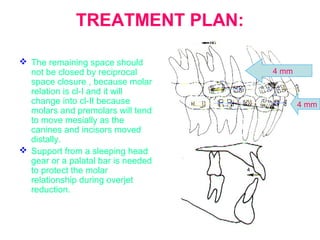
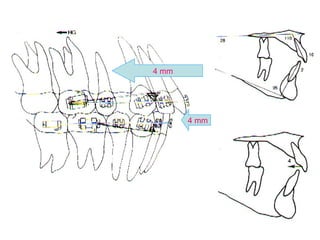
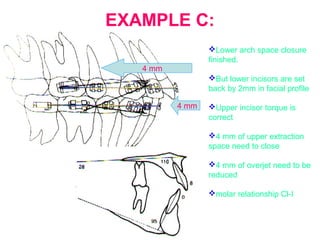
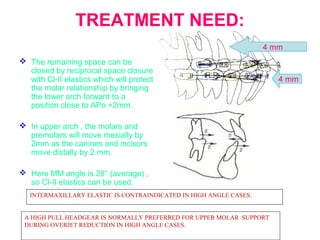
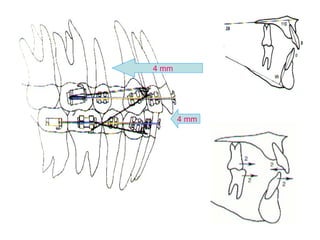
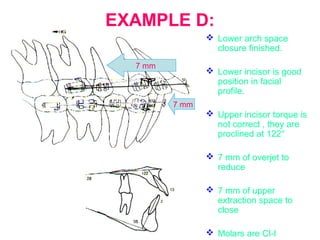
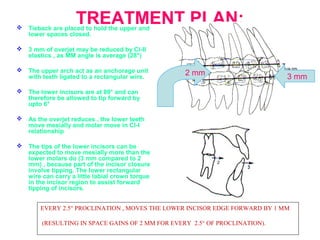
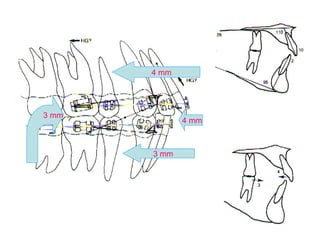
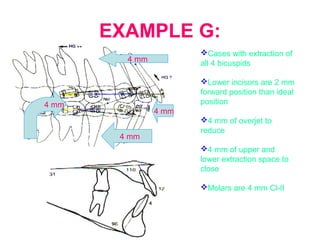
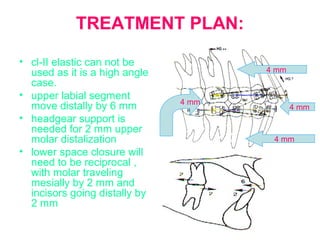
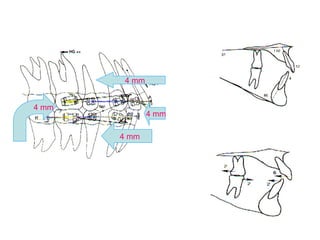
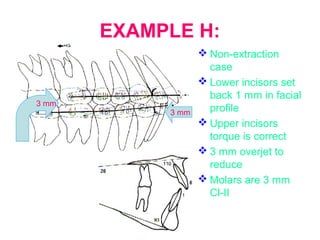
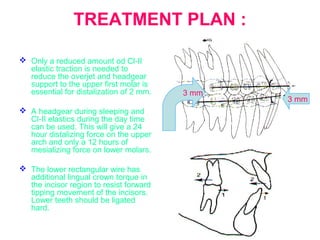
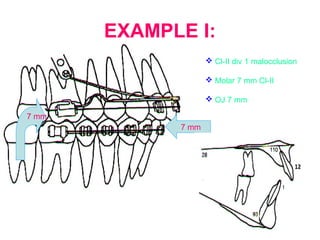
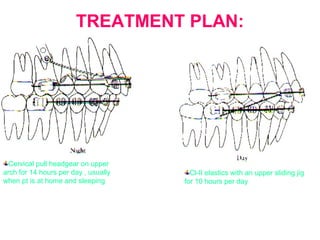
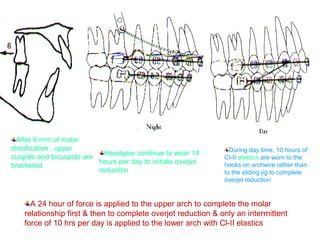
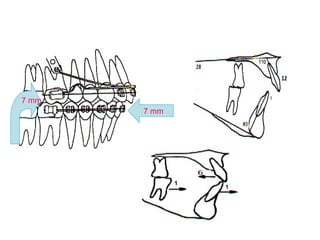

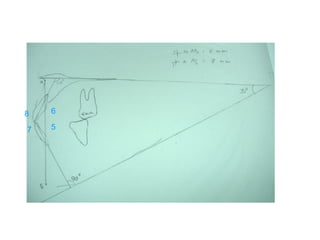








This document discusses strategies for reducing overjet in orthodontic treatment. It presents four examples of patients requiring overjet reduction and proposes treatment plans for each. The key points covered are the four main ways to reduce overjet: moving the lower incisors forward, moving the upper incisors back, moving the mandible forward, and limiting maxillary growth. Factors like molar relationship, amount of extraction, and facial angle are considered for determining the best mechanics in each case.








![FACEMASK CHINCUP SEMINAR[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/facemaskchincupseminar1-230916061625-e0964de8-thumbnail.jpg?width=640&height=640&fit=bounds)

























































