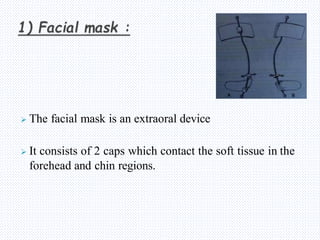
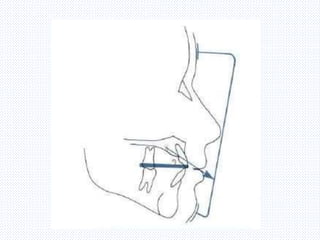
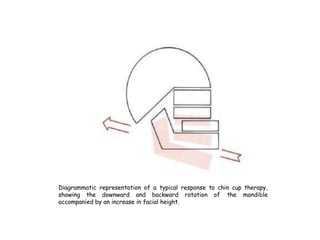
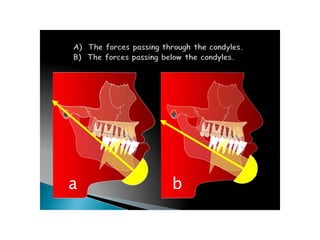
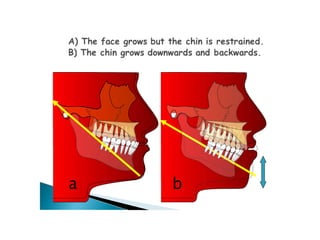
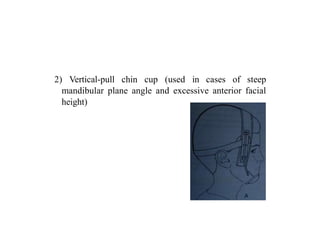
This document discusses facial masks and chin cups used in orthodontic treatment. It provides historical background on facial masks, describing their development over 100 years ago. It outlines the key components of orthopedic facial mask therapy, including the facial mask itself with forehead and chin caps connected by a metal frame, as well as intraoral appliances and elastic forces. The document discusses different types of facial masks and their indications, effects, and guidelines for use in treating Class III malocclusions and maxillary deficiencies. It also briefly covers chin cups and their effects of downward and backward rotation of the mandible.

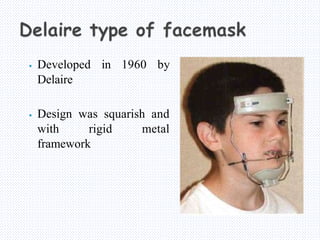
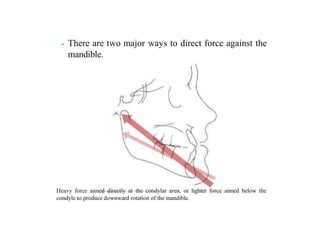





















































![REFINED BEGG philosophy [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/refinedbeggautosaved-240320080936-1a2298b4-thumbnail.jpg?width=640&height=640&fit=bounds)


































