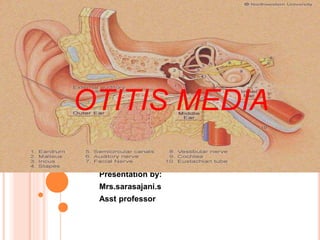
This document discusses otitis media, or middle ear infection. It begins by defining key terms related to ear diseases and infections. It then discusses the incidence, causes, risk factors, signs and symptoms, complications, diagnostic evaluation, and management of otitis media. Otitis media is most common in young children and is usually caused by bacterial or viral infections that obstruct the Eustachian tubes. Common symptoms include ear pain, fever, and hearing loss. Treatment involves antibiotics, anti-inflammatory drugs, or sometimes surgical drainage of fluid from the middle ear. Repeated infections can lead to permanent hearing loss or other complications if left untreated.