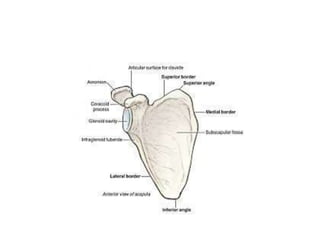
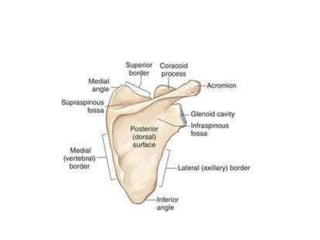
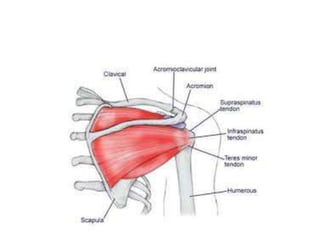
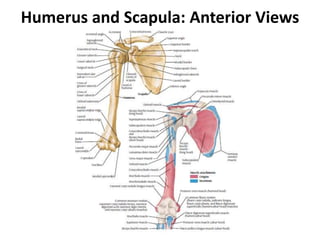
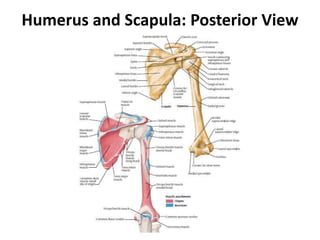
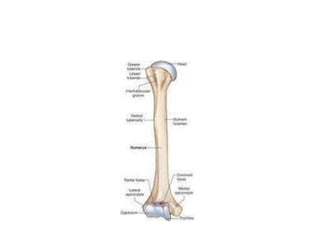
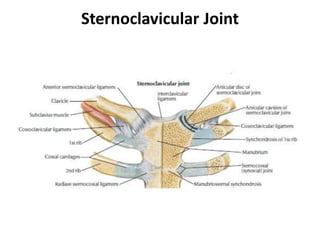
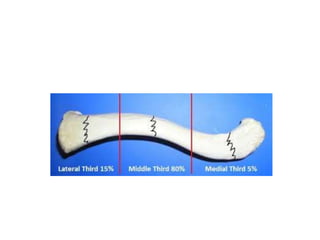
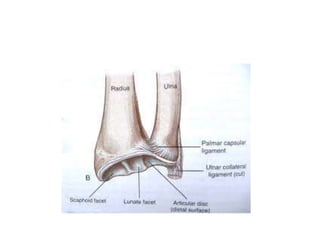
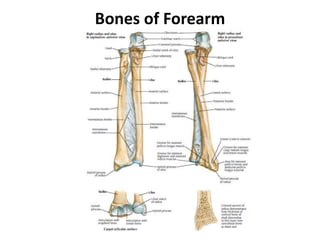
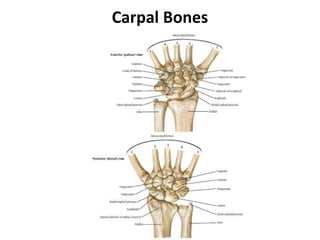
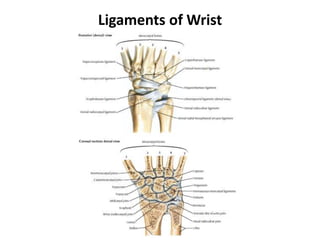
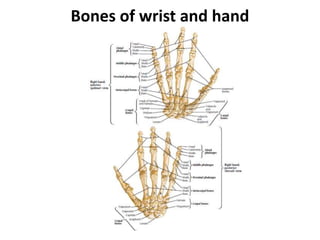
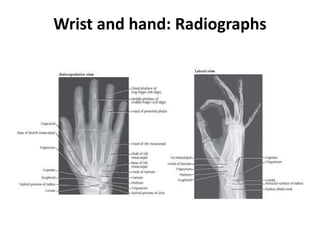
The document provides an overview of the osteology of the upper limb, including the scapula, clavicle, humerus, radius, ulna, carpal bones, metacarpals, and phalanges. It describes the anatomy of each bone including important structures, articulations, and clinical considerations such as common fractures. The upper limb bones form several joints including the shoulder, elbow, wrist, and finger joints which provide mobility to the arm.