
Recommended
More Related Content
What's hot
What's hot (20)
Similar to osseodensification-221027015308-2fae2d6f.pdf
Similar to osseodensification-221027015308-2fae2d6f.pdf (20)
More from Rutu Dabhi
More from Rutu Dabhi (17)
Recently uploaded
Recently uploaded (20)
osseodensification-221027015308-2fae2d6f.pdf
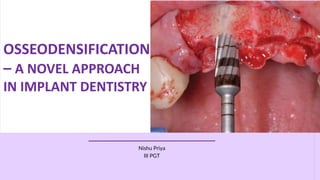
- 1. OSSEODENSIFICATION – A NOVEL APPROACH IN IMPLANT DENTISTRY Nishu Priya III PGT
- 3. Introduction Osseointegration is defined as a direct structural and functional connection between ordered, living bone and the surface of a load carrying implant. Osseointegration is crucial for implant stability which determines the long term success of dental implants. Albrektsson T et al., mentioned six major parameters like the implant material, implant surface, implant design, host factors, implant surgical technique and biomechanical factors which play a leading role in achieving osseointegration.
- 4. The main factor in implant placement is to achieve primary implant stability. The factors which are mainly involved in improving primary stability of dental implants are bone density, surgical protocol, implant thread type, and geometry. During osteotomy preparation, the maintenance and preservation of bone leads to enhanced primary mechanical stability and enhanced Bone to Implant Contact (BIC), thereby enhancing the implant secondary stability
- 5. Standard drill designs applied during osteotomies are made to excavate bone to create room for implant placement. They remove away the bone effectively however, typically do not produce a precise circumferential osteotomy. Unlike traditional bone drilling technologies, osseodensification does not excavate bone tissue. Osseodensification is a non extraction technique, which was developed by Huwais S . It is carried out with specially designed burs to increase bone density as they expand osteotomy site.
- 6. Primary and Secondary Stability This allows the implant to mechanically interlock with the bone tissue until secondary stability is achieved. A few factors which affect the implant stability are bone density, implant design, the Insertion Torque (IT) and the surgical technique. Due to surgical trauma, 1 mm of bone around the implant body gets devitalised, resorbed and remodelled in the initial period of osseointegration, this will decrease the primary stability. Later bone starts forming around implant body, thereby increasing the BIC. This biologic stability of the implant known as secondary stability leads to an osseointegrated implant. Primary stability is accomplished when there is no micromovement of implant in its completely seated position.
- 7. The primary stability on chair side can be evaluated by mobility using a blunt instrument such as a mirror handle and during follow-up visits, it can be estimated by devices such as periotest, periometer, Resonance Frequency Analysis (RFA), and placement torque. Meredith N et al., have shown Osstell™ transducer as a device used to evaluate the initial stability of a dental implant. It monitors the implant stability over time, and can discriminate clinical success and failures of implant. The osstell™ also allows the evaluation of an implant’s stability by resonance frequency. Another method to evaluate implant’s primary stability is the measure of the IT. Evaluation of primary stability
- 8. Principle of Osseodensification OD is a novel biomechanical bone preparation to place a dental implant, using burs (densah burs) which are rotated in reverse at 800 to 1500 rpm. Standard traditional drills remove and excavate bone during implant site preparation. Whereas, the new burs (densah burs) allow bone preservation and condensation through compaction autografting during osteotomy preparation thereby increasing the peri-implant bone density (% BV), and the implant mechanical stability. The rationale behind this process is the densification of the bone that will be in immediate contact to the implant results in higher degrees of primary stability due to physical interlocking between the bone and the device, faster new bone growth formation due to osteoblasts nucleating on instrumented bone that is in close proximity with the implant. The main concept of osseodensification technique is that the drill designing creates an environment which enhances the initial primary stability through densification of the osteotomy site walls by means of autografting of bone.
- 9. Consistent osteotomies and densification are considered to be vital for increased IT, implant primary stability, and early loading. Higher IT values and denser peri-implant bone together increase primary stability and healing and minimize implant micromotion. Trisi P et al., demonstrated that high IT in dense bone does not initiate bone necrosis or dental implant failure. Higher IT combined with enhanced OD of the implant site is desired. The science behind osseodensification concept Osseodensification (OD) technique generates a layer of condensed autograft along the surface of the osteotomy site where, there is bone paucity. The compacted, autologous bone immediately in contact with an endosteal device will have higher degrees of primary stability which also facilitate osseointegration. In conventional drills bone remodelling requires more than 3 months to repair the damaged area. Hence, Osseodensification (OD) technique help to reduce the healing period.
- 10. Mechanism of the osseodensification procedure In osseodensification (OD) procedure, the densifying burs produce a controlled bone deformation, which allows the expansion of a cylindrical osteotomy without excavating any bone tissue. When the osteotome is removed, the spring-back effect is a response of compacted bone that reduces the osteotomy to a smaller diameter. The spring-back phenomenon is due to the viscoelastic deformation. To achieve bone compaction Viscoelastic process is used.
- 11. What is Densah® and Versah® LLC? Dr. Salah Huwais in 2013 created Densah® Burs which were constructed by Versah® LLC company. Versah® able to provide unique and advance way of preparing osteotomies for implant placement. His aim was to preserve the healthy bone and make space. This led to the development of the new concept “Osseodensification (OD)” also called as “The Densah Technology by Dr. Huwais”. He invented specially designed burs called Densah burs.
- 12. Bur Technology Specially designed Densah burs precisely cut bone in the clockwise direction and densify bone in a non cutting counterclockwise direction combined with copious irrigation which facilitates the surgical technique during implant placement. The densah bur featuring multiple flutes within a tapered geometry is designed to produce a faster feed rate with less heat elevation. Densah burs on rotating counterclockwise, the flute back rake angle creates OD. Apart from that, operating at a counterclockwise speed, it is able to preserve bone and expand the bone to prepare the osteotomy for implant placement.
- 13. Technology behind the Densah® burs 1. These burs have a twist drills or straight fluted drills with four or more lands to guide them through the osteotomy and smoothly compact the bone. 2. It has many lands with a large negative rake angle, which work as non- cutting edges to increase the bone density as they expand an osteotomy in which the displaced bone is compacted and compressed circumferentially. 3. The pattern of burs have a cutting chisel edge and a tapered shank, so that they easily enter deeper into the osteotomy site, and controls the expansion process.
- 14. 4. These burs can used as a densify bone by rotating in the non-cutting direction (counter clockwise at 800 - 1,200 rotations per minute) or drill bone by rotating in the cutting direction (clockwise at 800 - 1,200 rotations per minute). The outward pressure combined with irrigation at the point of contact creates a hydrodynamic 2 compression wave so that the bone is compressed laterally by continuously rotating and concurrently forcibly advancing the bur. The taper design of the bur allows the operator to instantly lift away from contact to allow for irrigation. The tip design along with flutes facilitates compaction autografting.
- 15. Overview of Densah™ bur kit: 1. Kit is designed with 12 burs to create osteotomies. 2. Each Densah™ Bur is marked from 8 - 20 mm depth. 3. In dense bone, Densah™ Burs are designed in small increments (alternate between VT5 and VT8). 4. In soft bone, the osteotomy should be prepared by Densah™ Bur with an average diameter 0.5 - 0.8 mm. 5. In hard bone, the osteotomy should be prepared with Densah™ Bur with an average diameter 0.2 - 0.5 mm.
- 17. Healing of the osteotomy by osseodensification technique The most specific feature of the healing pattern is observed at the level of the coronal area where, the bone presented an granular aspect. In these zones, the bone trabeculae shows outer side lamellar bone layers and the specific granular layer in the inner side. The percentage of bone surface lined by osteoid bands in the coronal area is much higher than that found in other areas of the implants. The increase of bone density is particularly evident in the most coronal implant region. Active bone remodeling is found to be directed more toward bone apposition and bone density increase than toward bone resorption. This suggests that, in the long run, the bone could still increase its density.
- 18. Advantages of Osseodensification 1. Compaction autografting/condensation: OD maintains the bulk of bone by condensation which results in higher BIC. 2. Enhances bone density: In vitro testing reported that the densah burs allow bone preservation and condensation through compaction autografting during osteotomy preparation, increasing the peri-implant bone density (BV%), and the implant mechanical stability. 3. Residual ridge expansion 4. Increases residual strain: create a rate-dependent stress to produce a rate dependent strain, and allows saline irrigation to gently pressurise the bone walls. 5. Increases Implant Stability 6. Higher insertion torque values due to osseodensification result in good prognosis. Contraindications of Osseodensification 1. Mentioning the contraindications, OD does not work with cortical bone as cortical bone is a non dynamic tissue which lacks plasticity. 2. Densification of xenografts should be avoided because they behave biomechanically different than the bone tissue, as they have only inorganic content and they just provide the bulk without any viscoelasticity. Limitations 1. Osseodensification (OD) does not work with cortical bone as cortical bone lacks plasticity. 2. Prevent the densification of xenografts.
- 19. Indications 1. It facilitates lateral ridge expansion- Ridge with less than 3 mm of width. 2. It facilitates vertical ridge expansion in maxillary sinus. Contraindications 1. Patients with various systemic disorders such as compromised immune system, bleeding disorders and titanium allergy should be excluded.
- 20. DISCUSSION Lahen B et al., in their study examined the effect of OD on the primary stability and early osseointegration of implants. Their results showed that the OD drilling technique significantly enhanced IT values which are considered in this study as a method to gauge device primary stability. After six weeks in vivo, histometric results suggest that the experimental groups drill design positively influenced osseointegration when utilized in both clockwise or counterclockwise (OD) directions. Thus they concluded that regardless of the design of the of implant, the OD drilling technique enhanced the primary stability and BIC. They also concluded it as a result of the densification of autologous bone debris at the bone walls.
- 21. Trisi P et al., evaluated the efficacy of OD technique to enhance bone density of ridge, width and implant secondary stability. They conducted a biomechanical and histological analysis after inserting 20 implants in the iliac crest of two sheep and using conventional drill for implants on one side as control and OD for implants on the other side as test group. They reported a significant increase in ridge width and bone volume percentage of 30% in the test group. This increase of bone density in the OD site was said to be evident in the most coronal implant site where the bone trabeculae were thickened because of incorporation of autogenous bone fragments during healing. In conventional osteotomy, the surgical technique influences the BIC which has an effect on osseointegration. Bone sacrifice and trabeculae fracture is unavoidable with conventional osteotomy, which delays the bone growth. In OD technique, maintaining and preserving bone leads to increased primary stability, increased BIC, which in turn enhances implant secondary stability and fastens healing and remodelling. The bone trabeculae get thickened due to the incorporation of autogenous bone fragments, during healing process. Lopez CD et al., in their study assessed the biomechanical and histological effects of OD surgical instrumentation in a spine model animal study and concluded that this technique can potentially improve the safety and success rates of bony drilling at all sites of low bone density and limited bone volume.
- 22. A 60-year-old healthy female visited the outpatient ward (OP) of a tertiary care referral hospital to have an implant placed in her left maxillary first molar region. A cone-beam computed tomography (CBCT) scan showed that there were root-stumps in that region requiring extraction; also, it was observed that the floor of the sinus was very close to the alveolar crest.
- 23. The root stumps were removed and the socket was preserved with demineralized freeze-dried bone allograft. Six months post-extraction, the patient visited the OP for implant placement. CBCT scan of the left upper first molar region taken preoperatively before the surgical procedure.
- 24. As the ridge height from the sinus floor to the alveolar crest was 5 mm, it was decided to go ahead with a crestal sinus lift to enable the placement of a 5 mm x 8 mm implant.
- 25. The clinical picture showing the edentulous site in relation to the left upper first molar, taken preoperatively Then the flap was elevated using mid crestal and crevicular incisions. The osteotomy was started with the pilot drill in clockwise mode 1 mm short of the sinus floor. A 2.5 mm Densah™ bur (Jackson, MI: Versah, LLC) at 800 rpm speed in an anticlockwise direction was inserted 1 mm short of the sinus floor.
- 26. Sequential widening using 3 mm, 3.5 mm, and 4 mm was done, changing the drill motor to reverse- densifying mode with a gentle pumping motion following the manufacturer’s instructions. Additional vertical depth and membrane lift were achieved in the process. Intermittent pressure of one second off and on the bone, under copious saline irrigation was followed throughout the procedure. The final 4.5 mm drill was inserted only half the depth of the osteotomy to attain primary stability. The image is showing RVG taken immediately after implant placement. amount of sinus lift (3.01 mm) achieved, by osseodensification burs, facilitating the placement of a 5 x 8 mm implant without traumatizing the sinus.
- 27. The image is showing RVG taken three months after implant placement. The clinical picture taken three months post-implant placement is showing the healing abutment tightened over the implant.
- 28. Discussion The conventional osteotomy preparation protocol revolves around removing the bone to suit the implant being placed, thus reducing the insertion torque leading to poor primary stability and potential lack of integration. The novel osseodensification approach on the other hand uses burs with numerous grooves and increasing diameters in the anticlockwise direction, which favorably reduces the implant bed preparation, thus increasing the stability of the placed implant. Because of the counter-clockwise direction of these burs, it is hypothesized that there would be autogenous bone compaction at the apical end which facilitates gentle lifting of the sinus membrane. Using the osseodensification burs for a sinus lift is a minimally invasive procedure that negates the placement of graft material after sinus augmentation. It has been reported in a very recent systematic review that there was an increase in BIC and bone area fraction occupancy (BAF). Moreover, osseodensification technique has been demonstrated to increase the bone volume percentage around dental implants inserted in atrophic bone, with respect to the conventional implant drilling techniques, thus reducing the micromotion and enhancing implant stability.
- 29. Conclusion This case report describes the benefits of using osseodensification burs (Densah™) for sinus augmentation as well as implant site preparation. This protocol is best followed when the preferred sinus lift is ≤ 3 mm. Osseodensification is a very promising minimally invasive tool for crestal approach of sinus augmentation. However, longitudinal studies with larger samples are to be done to assert its role in sinus augmentation procedures.
- 30. The patient is a 62-year-old male presented with missing teeth Nos. 19, 20, and 21. Clinical and radiographic examination revealed a significant alveolar ridge resorption, which resulted in a Seibert Class I, ridge deficiency. The patient’s medical history was noncontributory.
- 31. Treatment options with their potential risks and benefits were presented to the patient. A final treatment plan was finalized to utilize placement of two implants to receive two abutments for a fixed prosthesis to restore teeth Nos. 19, 20, and 21 Lower left area was anesthetized using infiltration method with 1.8 ml 4% Septocaine® (Septodont) with 1:100,000 epinephrine. Once anesthetized, crestal incision was done, and full thickness flap was reflected to reveal 2.5 mm- 3.0 mm crestal alveolar ridge width, which was confirmed by direct measurement
- 32. The site preparation for two implants in the areas of Nos. 19 and 21 began with site marking. Then, a 1.5-mm initial pilot osteotomy was created with a pilot drill rotated at 1200 RPM in a clockwise rotation (CW) to a depth of 13 mm utilizing a highspeed surgical handpiece and a surgical Motor (W&H). Once implant positions were confirmed, a horizontal ridge split to a 10-mm depth was created using Piezosurgery® (Piezosurgery Incorporated) to allow further buccal plate flexibility. Osseodensification with ridge expansion started with Densah™ Bur VT1525 (Versah™, LLC) rotating in a non-cutting counterclockwise (CCW) direction at 1200 RPM (Densifying Mode) to expand the osteotomy to 2.5 mm, utilizing a high-speed surgical handpiece and a surgical Motor (W&H)
- 33. Then Densah™ Bur VT2535 (Versah, LLC) running in a non-cutting counterclockwise (CCW) direction at 1200 RPM (Densifying Mode), utilizing a high-speed surgical handpiece and a surgical Motor (W&H), was used to expand osteotomies in the area of implant Nos. 19 and 21. Mandibular osteotomies were expanded to 3.5 mm without any bone dehiscence, which then allowed for total implant length placement in autogenous bone without any threads exposure.
- 34. Two 3.7/13 Tapered Screw-Vent implants (Zimmer®) were placed with an insertion torque of 40-50 Ncm. Both implants total lengths were covered with autogenous bone. Less than 1.0 mm crestal-buccal bone thickness in area of implant No. 21 was noted. Implant stability was measured with an (Osstell®) ISQ implant stability meter, which uses resonance frequency analysis. In this particular case buccal-lingual ISQ readings in the areas of Nos. 19 and 20 were 78 and 49, respectively. Several studies have been conducted on resonance frequency analysis (RFA) measurements and the ISQ. They provided valid indication that accepted stability range is above ISQ 50 and recommended loading at ISQ 67-68.
- 35. Due to ISQ reading of 49 in the mesial implant No. 21 and less than 1.0 mm of crestal-buccal bone thickness remaining after osseodensification, the decision was made to augment the buccal plate with bone graft.
- 36. Eight weeks post placement, implants were uncovered through shallow crestal incision. Healing abutments were placed. Buccal-lingual ISQ readings obtained at week 10 were 76/72, 67 for implant Nos. 19 and 20, respectively. Implants high insertion torque with maintained gain in ISQ had allowed us to consider an early restorative phase initiation. Thus, at 10 weeks, when ISQ reading reached ≥ 67, the patient was referred back to his restorative dentist for the restorative phase
- 37. Fourteen weeks post implant surgery, a fixed prosthesis retained by implants Nos. 19 and 21 was delivered.
- 38. Supportive and follow-up care Patient returned in 1 year for clinical and radiographic follow-up. Examination revealed healthy hard and soft tissue with no sign of inflammation or infection. Radiographic examination revealed maintained crestal bone level and bone density. Clinical examination revealed slight soft tissue recession in the area of implant No. 21. This soft tissue height reduction is common post GBR or ridge augmentation procedures. Four months’ interval supportive periodontal treatment was initiated with yearly radiographic examination for implant Nos. 19 and 21.
- 40. In this case, osseodensification utilizing the Densah™ Bur technology had facilitated ridge expansion with maintained alveolar ridge integrity, allowing for total implant length placement in autogenous bone with adequate primary stability. Despite compromised bone anatomy, osseodensification preserved bone bulk and promoted a shorter waiting period to the restoration. Ordinarilly, a case similar to this patient would progress through three phases of treatment over 30- 50 weeks: 1. Ridge augmentation phase (6-9 months) to increase ridge width with either block grafting or guided bone regeneration 2. Implant placement and healing phase (2-3 months) 3. Restorative phase The question remains, why do we build bone bulk to then extract it later and wait months for implants to heal? It is time to think about bone preservation to enhance its ability to heal faster, regardless of implant macro- or micro-geometry.
- 41. Most of the techniques suggested for implant osteotomy involve removal of bone. Osseodensification (OD) has recently been introduced, as a new osteotomy technique, which enhances implant stability. This technique reduces bone sacrifice that appears inevitable with conventional drilling procedures. The concept of osseodensification (OD) has changed the prototype of implant site preparation and is found to be beneficial in creating a stronger expanded osteotomy for implant placement, through compaction and autografting. This technique is shown to increase the primary stability, bone mineral density, and the percentage of bone at the implant surface. The healing process will be enhanced by preserving the bone bulk. Current literature evidence is inadequate to draw any concrete conclusion, and more long-term clinical trials and randomized controlled studies are recommended in this field for high level evidence. Conclusion and Future Perspective
- 42. References 1. Misch CE: Rationale for dental implants. Dental Implant Prosthetics. Second Edition. Elsevier Mosby, St. Louis, MO; 2015. 1-25. 2. Rodda A, Koduganti R R, Manne H K, et al. (January 31, 2022) Implant Placement Post Maxillary Sinus Lift Using Osseodensification Concept: A 3. Case Report. Cureus 14(1): e21756. DOI 10.7759/cureus.21756 4. Jackson CJ, Ghosh SK. On the evolution of drill-bit shapes. Journal of Mechanical Working Technology. 1989;18(2):231-267. 5. Natali C, Ingle P, Dowell J. Orthopaedic bone drills-can they be improved? Temperature changes near the drilling face. J Bone Joint Surg Br. 1996;78(3):357-362. 6. Frost HM. A brief review for orthopedic surgeons: fatigue damage (microdamage) in bone (its determinants and clinical implications). J Orthop Sci, 1998;3(5):272-281. 7. EG, Huwais S. Osseodensification Is A Novel Implant Preparation Technique That Increases Implant Primary Stability By Compaction and Auto-Grafting Bone. American Academy of Periodontology. [abstract]. San Francisco, CA. 2014. 8. Albrektsson T, Zarb G, Worthington P, Eriksson AR. The long-term efficacy of currently used dental implants: A review and proposed criteria of success. Int J Oral Maxillofac Implants. 1986;1(1):11-25.