Downloaded 289 times

![TREATEMENT OF MDR T.B.
RNTCP Regimen for MDR TB: 6 (9) Km Lvx Eto Cs Z E / 18 Lvx Eto Cs E
[Reserve/Substitute drugs: PAS, Mfx, Cm]
TREATEMENT OF XDR T.B.
RNTCP Regimen for XDR TB: 6-12 Cm, PAS, Mfx, High dose-H, Cfz, Lzd, Amx/Clv
/ 18 PAS, Mfx, High dose-H, Cfz, Lzd, Amx/Clv [Reserve/Substitute drugs:
Clarithromycin, Thiacetazone]](https://image.slidesharecdn.com/rntcp-160207043609/85/RNTCP-26-320.jpg)
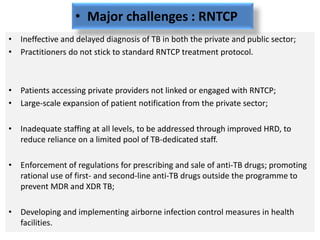

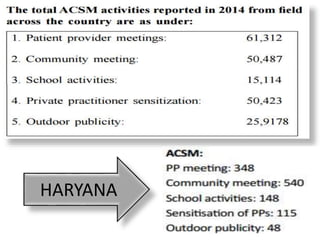


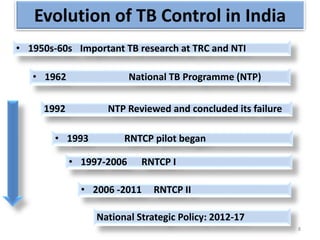
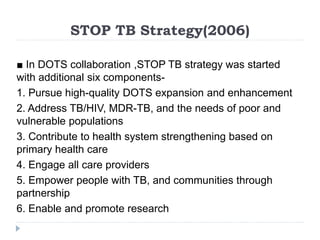
The document summarizes India's Revised National Tuberculosis Control Programme (RNTCP). Some key points: 1) RNTCP was established in 1993 to address the failures of the previous National Tuberculosis Programme, such as low treatment completion rates. RNTCP's goals are to reduce TB mortality and interrupt transmission. 2) RNTCP follows the DOTS strategy - ensuring political commitment, quality diagnosis, quality drugs, direct observation of treatment, and systematic monitoring. It has treatment categories based on patient type with standardized regimens. 3) Major achievements include treating over 19 million patients since inception and achieving case detection and treatment success rates in line with global targets. However, challenges remain such as ineffective private


































































