Download to read offline













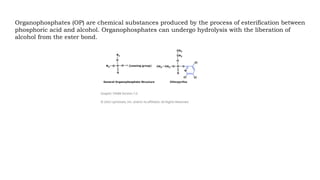
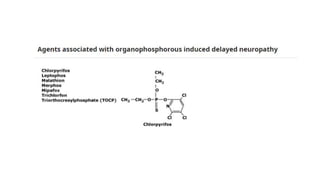


The document discusses the history, pathophysiology, and treatment of organophosphate poisoning, primarily due to insecticide exposure. It outlines the effects of acute and delayed symptoms, complications, and diagnostic approaches, as well as treatment considerations such as decontamination and the use of antidotes. Carbamate insecticides, while similar in acute effects, have different mechanisms and treatment protocols, with the importance of protective measures highlighted throughout.




















































































