Download to read offline


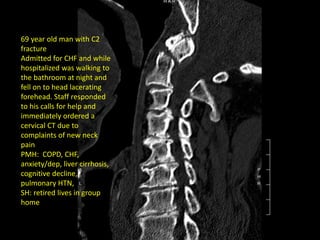





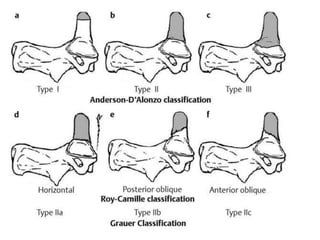

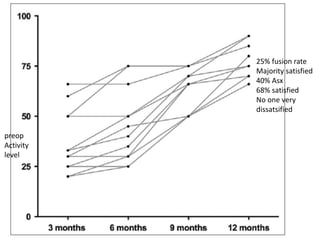
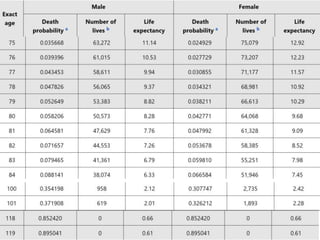
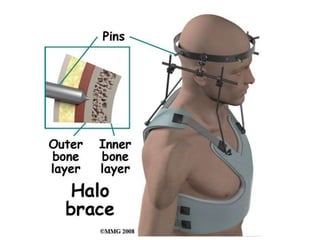
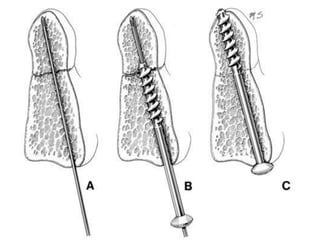
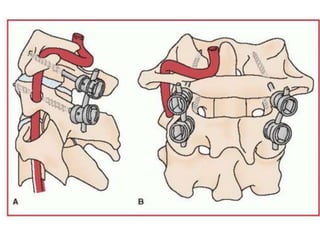
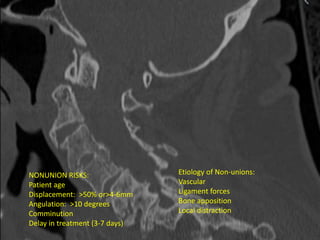
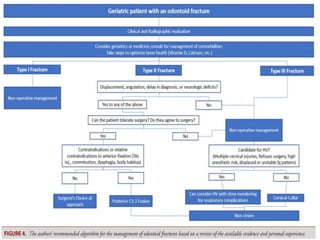
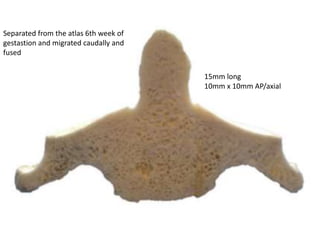
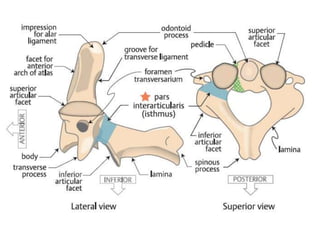
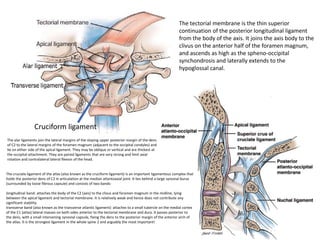
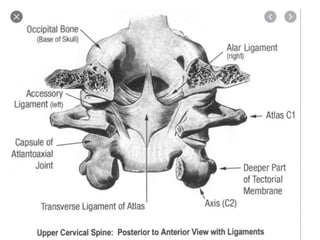
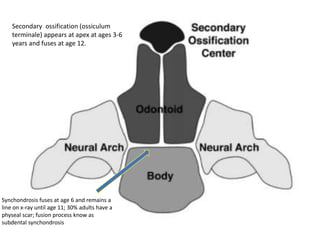
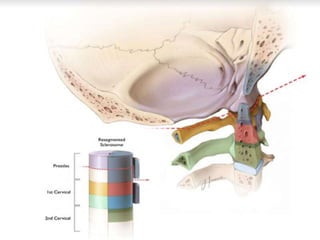
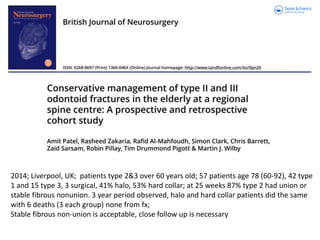
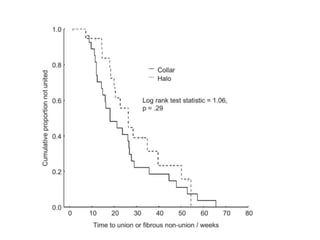
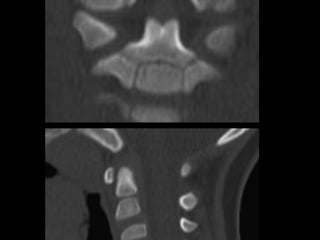


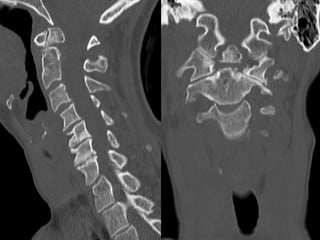

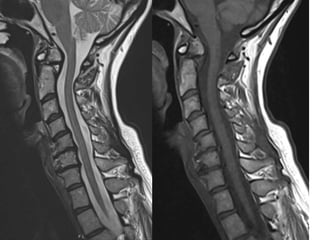

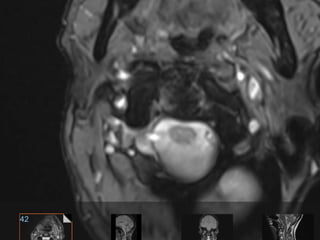




This document discusses odontoid fractures and their treatment. It provides details on the anatomy of the odontoid process (C2 vertebra) and describes a case of a 69-year-old man who fell and suffered a C2 fracture. It then reviews literature on outcomes of operative versus non-operative treatment of odontoid fractures in older patients, finding that operative patients had longer hospital stays but lower mortality rates. Risk factors for non-union of odontoid fractures are discussed. The document also provides further anatomical details on ligaments surrounding the C1-C2 vertebrae.























































































