CONTENTS
CONTENTS
• Introduction
• History
•Various types of artificial eyes
• Patient evaluation
• Fabrication of ocular prosthesis
• Post insertion care of ocular prosthesis
• Conclusion
• References
4.
INTRODUCTION
INTRODUCTION
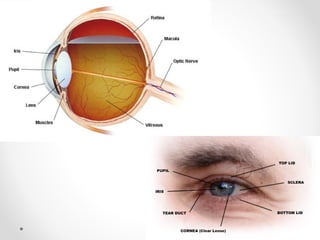
OCULAR PROSTHESIS: amaxillofacial prosthesis that
artificially replaces an eye missing as a result of trauma,
surgery, or congenital absence. The prosthesis does not
replace missing eyelids or adjacent skin, mucosa or
muscle. (GPT – 8)
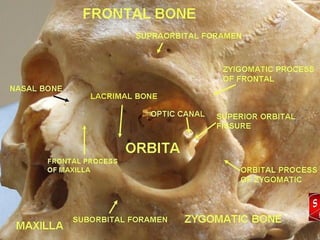
Muscular attachment of
Muscularattachment of
normal eye
normal eye
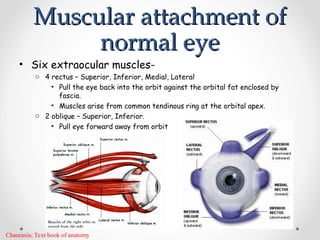
• Six extraocular muscles-
o 4 rectus – Superior, Inferior, Medial, Lateral
• Pull the eye back into the orbit against the orbital fat enclosed by
fascia.
• Muscles arise from common tendinous ring at the orbital apex.
o 2 oblique – Superior, Inferior.
• Pull eye forward away from orbit
Chaurasia; Text book of anatomy
8.
HISTORY
HISTORY
• Use of“ART EYES” in statues by Egyptians (1613-2494 BC)
• Ambroise Pare (1510-1590) –first to describe the use of
artificial eyes in fitting an eye socket ( pioneer of modern
artificial eyes)- fabricated eyes of porcelain.
S. B. Patil et al. Ocular prosthesis: a brief review and fabrication of an ocular prosthesis for a geriatric patient.
Gerodontology 2008; 25: 57–62
9.
• Ludwig Muller-Uri(1830’s)-glass eyes.
• Frohlich and Van Duyse (1884) – tried using ivory,
valcunite and celluloid.
• II World war-Naval dental school(1943)- use of
acrylic resin – superior to glass.
S. B. Patil et al. Ocular prosthesis: a brief review and fabrication of an ocular prosthesis for a geriatric patient.
Gerodontology 2008; 25: 57–62
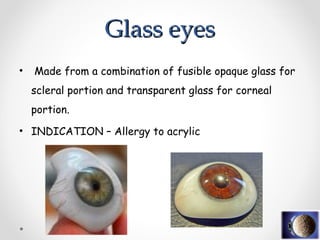
• Made froma combination of fusible opaque glass for
scleral portion and transparent glass for corneal
portion.
• INDICATION – Allergy to acrylic
Glass eyes
Glass eyes
12.
• Becomes roughand looses its transparency.
• Easily fractured.
• More liable to get scratched.
Poor fusion can produce cracks ocular secretions
gather inside increased weight.
• Difficult to fit properly in relation to defect.
• Color of the iris of the glass looses its glaze and
becomes dim over years.
Disadvantages
Disadvantages
13.
Acrylic resin eyes
Acrylicresin eyes
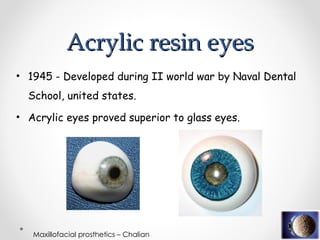
• 1945 - Developed during II world war by Naval Dental
School, united states.
• Acrylic eyes proved superior to glass eyes.
Maxillofacial prosthetics – Chalian
14.
• Compatible withtissues.
• Easy to work with.
• Easy color modification abilities – enhanced esthetics.
• No surface roughness due to socket secretions.
• Non fragile.
• Can be either preformed or custom made therefore can fit in a
better manner in the socket.
• Can be constructed with materials and equipments commonly
found in dental lab.
• Can be repolished to original shine and smoothness.
Advantages
Advantages
Maxillofacial prosthetics – Chalian
15.
CUSTOM OCULAR PROSTHESIS
CUSTOMOCULAR PROSTHESIS
• Close adaptation to the tissue bed
• Increased mobility of the prosthesis
• Distributes pressure more equally thus reduce the incidence of
ulceration
16.
• Enhances tissuehealth by reducing the potential stagnation spaces
at the prosthetic tissue interface (these voids collect mucous and
debris which can irritate mucosa and act as potential source of
infection).
• Improved facial contours
• Enhanced esthetics gained from control over the size of the iris,
color of the iris and sclera.
17.
STOCK OCCULAR PROSTHESIS
STOCKOCCULAR PROSTHESIS
• Disadvantages:
1. Though less time required but results are not
satisfactory.
2. Some discomfort always present.
3. Adaptation not very good:-
Movement compromised
Collection of mucosa and debris
18.
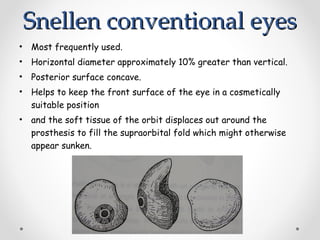
Snellen conventional eyes
Snellenconventional eyes
• Most frequently used.
• Horizontal diameter approximately 10% greater than vertical.
• Posterior surface concave.
• Helps to keep the front surface of the eye in a cosmetically
suitable position
• and the soft tissue of the orbit displaces out around the
prosthesis to fill the supraorbital fold which might otherwise
appear sunken.
19.
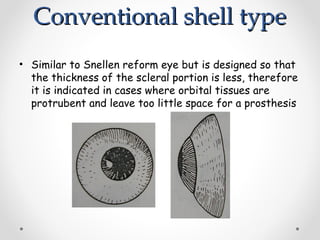
Conventional shell type
Conventionalshell type
• Similar to Snellen reform eye but is designed so that
the thickness of the scleral portion is less, therefore
it is indicated in cases where orbital tissues are
protrubent and leave too little space for a prosthesis
20.
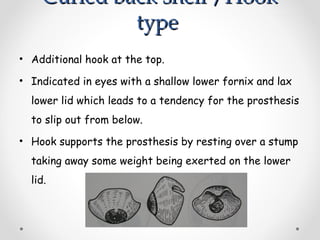
Curled back shell/Hook
Curled back shell /Hook
type
type
• Additional hook at the top.
• Indicated in eyes with a shallow lower fornix and lax
lower lid which leads to a tendency for the prosthesis
to slip out from below.
• Hook supports the prosthesis by resting over a stump
taking away some weight being exerted on the lower
lid.
21.
Patient evaluation
Patient evaluation
•Physical and Psychological evaluation
• Generally patients will present with either a conformer or
an existing prosthesis. remove and do thorough
examination of the defect.
Post surgical edema present wear conformer
Inadequate healing
Dehiscence over the implant
Presence of infection
Patil et al; Ocular prosthesis for geriatric patients. Gerodontology 2008, 25 ; 57-62
Taylor; Clinical maxillofacial prosthetics
22.
Socket examination:
• Todetermine presence of an implant and degree of mobility
• Presence of Cicatricial bands
• Internal anatomy of the socket
• Presence of tissue undercuts
• Depth of fornices
• Observation of the relations of the palpebral fissure in an
open and closed position.
Patil et al; Ocular prosthesis for geriatric patients. Gerodontology 2008, 25 ; 57-62
Taylor; Clinical maxillofacial prosthetics
23.
Etiology of eyeloss
Etiology of eye loss
• Malignancy
• Trauma
• Infection
• Blind, fragmented eye with growth and
• End stage glaucoma
Patil et al; Ocular prosthesis for geriatric patients. Gerodontology 2008, 25 ; 57-62
Taylor; Clinical maxillofacial prosthetics
24.
Surgical procedures inthe removal of eye are classified into three
categories:
•Evisceration : Surgical procedure wherein the intraocular
contents of the globe are removed, leaving the sclera, Tenon’s
capsule, conjunctiva, extraocular muscles and optic nerve are
undisturbed; the cornea may be retained or excised
•Enucleation :surgical removal of the globe and a portion of the
optic nerve from the orbit.
•Exenteration :en bloc removal of the entire orbit, usually
involving partial or total removal of the eyelids, and is performed
primarily for eradication of malignant orbital tumour
Eidz Kale, A technique for fabrication of an interim ocular prosthesis. Journal of prosthodontics.
2008, 654-661
25.
Orbital implants
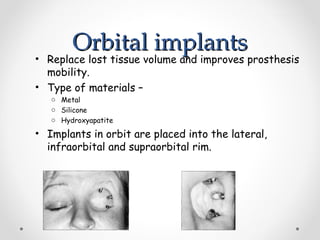
Orbital implants
•Replace lost tissue volume and improves prosthesis
mobility.
• Type of materials –
o Metal
o Silicone
o Hydroxyapatite
• Implants in orbit are placed into the lateral,
infraorbital and supraorbital rim.
26.
• Extraocular musclesattached to implant through
loop or screen on Implant, which allows for location of
suture placement.
• Muscle attachment is in the form of a crossed notch
on the anterior surface of the implant into which the
extraocular muscles can be placed and sutured
together
Fabrication Of Ocular
FabricationOf Ocular
Prosthesis
Prosthesis
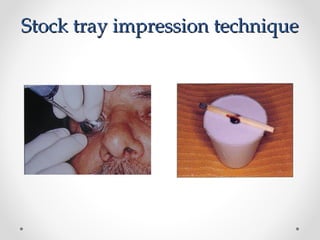
• Impression making
o Stock tray impression technique
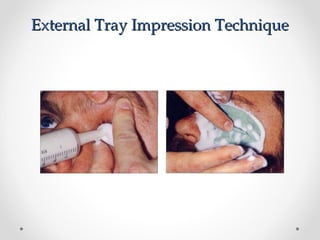
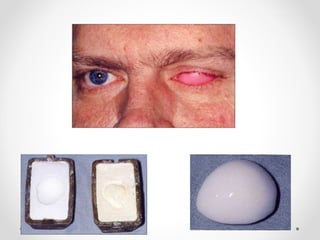
o External tray technique
• Selection of iris components
o Paper iris disk technique
o Black iris disk technique.
SELECTION OF IRISCOMPONENTS
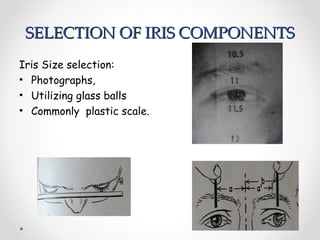
SELECTION OF IRIS COMPONENTS
Iris Size selection:
• Photographs,
• Utilizing glass balls
• Commonly plastic scale.
35.
Paper Iris DiskTechnique
Paper Iris Disk Technique
When the wax pattern is determined to be appropriate,
it is flasked and processed in scleral resin. The
scleral blank is then finished, and it is polished using
pumice and acrylic resin polish
36.
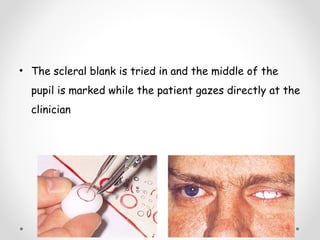
• The scleralblank is tried in and the middle of the
pupil is marked while the patient gazes directly at the
clinician
37.
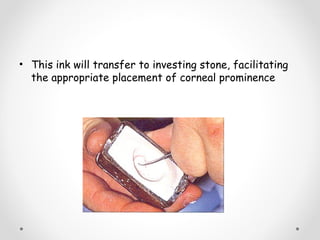
• This inkwill transfer to investing stone, facilitating
the appropriate placement of corneal prominence
38.
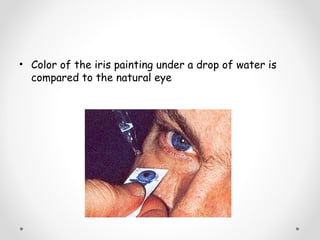
• Color ofthe iris painting under a drop of water is
compared to the natural eye
39.
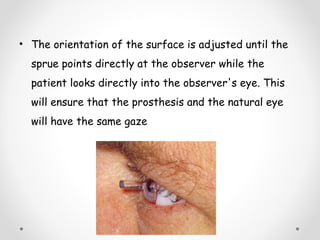
• The orientationof the surface is adjusted until the
sprue points directly at the observer while the
patient looks directly into the observer's eye. This
will ensure that the prosthesis and the natural eye
will have the same gaze
40.
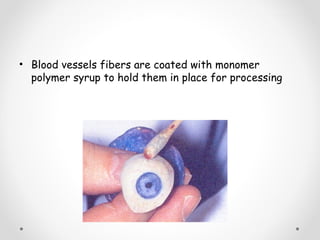
• Blood vesselsfibers are coated with monomer
polymer syrup to hold them in place for processing
41.
Black Iris DiskTechnique
Black Iris Disk Technique
• Patient position
• Ocular discs
which are used in iris painting, are available in half-
mm size increments, ranging from 11 mm to 13 mm
• Corneal buttons
Are available in the same size as the disc.
• Windsor newton oil pigments
42.
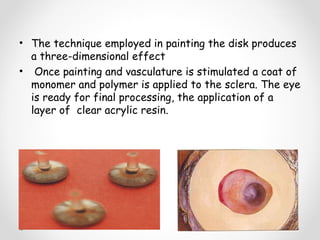
• The techniqueemployed in painting the disk produces
a three-dimensional effect
• Once painting and vasculature is stimulated a coat of
monomer and polymer is applied to the sclera. The eye
is ready for final processing, the application of a
layer of clear acrylic resin.
43.
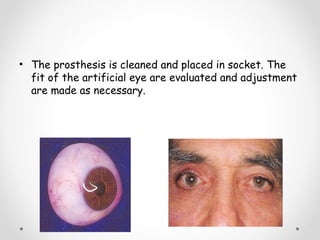
• The prosthesisis cleaned and placed in socket. The
fit of the artificial eye are evaluated and adjustment
are made as necessary.
44.
POST INSERTION AND
POSTINSERTION AND
INSTRUCTION AND CARE
INSTRUCTION AND CARE
1. Never clean or soak artificial eye in rubbing alcohol
because it will crack and destroy the ocular
prosthesis.
2. Remove the ocular prosthesis only as necessary. Too
much handling can cause socket irritation and result
in excessive secretions.
3. If Ocular prosthesis is removed it should be, stored
in water or soft contact lens saline solution. This will
keep deposits from drying on the surface.
45.
4. To cleanprosthesis, use an antibacterial soap. Wash
the eye between your fingertips.
5. Any eye drops can be used with the artificial eye in
place.
6. Patient to be recalled every 6 months.
46.
Conclusion
Conclusion
• The lossof eye requires early replacement so that the patient
may return to a normal life. Prosthetic rehabilitation is enhanced
if an implant is placed in the orbit
• Most patients benefit from custom made ocular prosthesis that
are modified to the individual needs. This approach is more time
consuming but the esthetic and functional results are better
with this technique.
47.
• The disfigurementresulting from the loss of eye can
cause significant psychological as well as social
consequences. With the advancement in Ophthalmic
surgery and ocular prosthesis , patients can be
rehabilitated very effectively
48.
References
References
• Maxillofacial prosthetics– Chalian
• Clinical maxillofacial prosthetics – Taylor
• Essentials of human anatomy – A.K.Dutta
• S. B. Patil et al. Ocular prosthesis: a brief review and fabrication of an
ocular prosthesis for a geriatric patient. Gerodontology 2008; 25: 57–
62
• Eidz Kale, A technique for fabrication of an interim ocular prosthesis.
Journal of prosthodontics. 2008, 654-661
• Kenneth Adisman . Custom ocular prosthetics; December 1982 volume
48 number 6