Download as PDF, PPTX

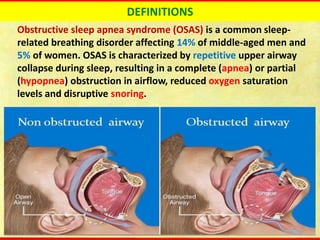



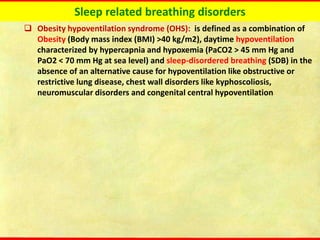
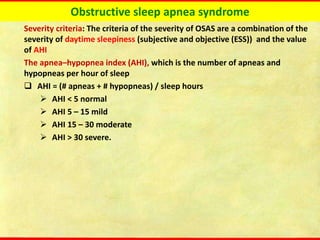
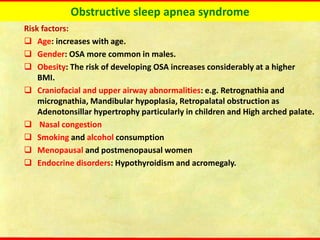
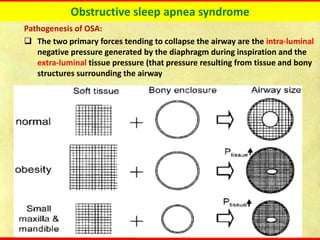
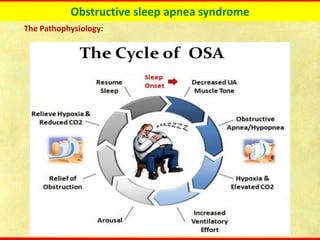
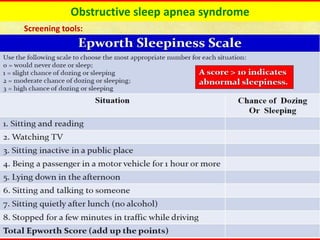
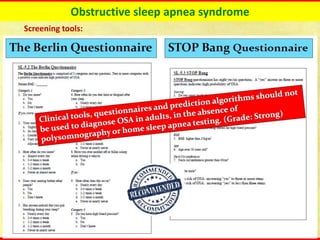






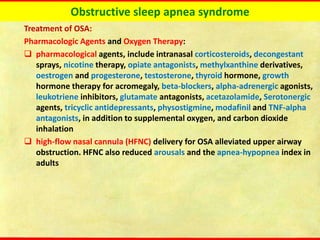

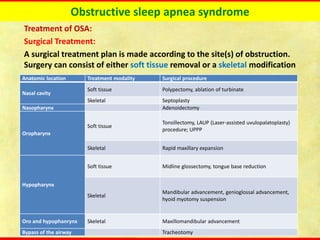

Obstructive sleep apnea syndrome (OSAS) is a common sleep disorder characterized by repetitive collapse of the upper airway during sleep, resulting in reduced airflow and oxygen levels. It affects 14% of middle-aged men and 5% of women. Polysomnography is the gold standard test used to diagnose OSAS and measure its severity based on the apnea-hypopnea index. Positive airway pressure therapy is the primary treatment, while other options include oral appliances, surgery, and lifestyle changes. Untreated OSAS can cause serious health complications.
































![OBSTRUCTIVE SLEEP APNEA [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/obstructivesleepapneaautosaved-240801041633-6b724373-thumbnail.jpg?width=640&height=640&fit=bounds)











































