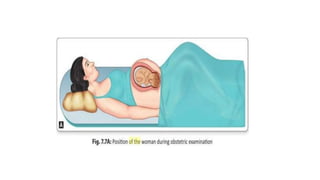
The document is a comprehensive guide on obstetric examinations during pregnancy, detailing essential preparatory steps, general and specific examination techniques including abdominal and vaginal assessments, and parameters for monitoring fetal health. It emphasizes the importance of consent, privacy, and comfort for the patient, while outlining methods for evaluating vital signs, fetal positioning, and estimating fetal weight. It includes various techniques like Leopold's maneuvers for determining fetal engagement and discusses the use of different instruments for auscultation of fetal heart sounds.