Downloaded 44 times









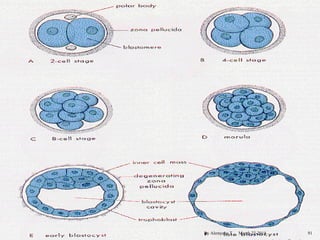
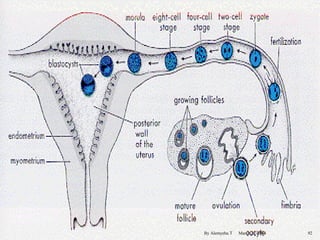
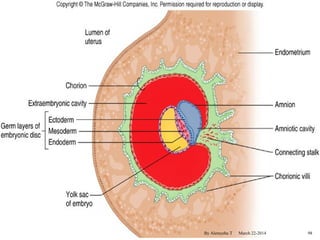


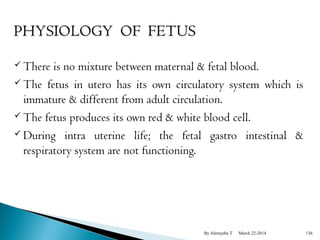




The document provides an overview of physiological changes during pregnancy presented by Alemyehu T. It describes changes in various body systems including increased blood volume, cardiac output and relaxed smooth muscles. Key stages of development are defined, from fertilization to implantation of the embryo. Major organ changes are also summarized such as uterine enlargement and breast development in preparation for lactation.














































![Physiological and psychological changes during pregnancyhanges [Recovered].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ppchangesrecovered-240119155912-065d14b8-thumbnail.jpg?width=640&height=640&fit=bounds)






















![Meas.association [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/meas-150203110718-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)


![Evaluation of evidence [compatibility mode]](https://cdn.slidesharecdn.com/ss_thumbnails/evaluationofevidencecompatibilitymode-150203110719-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




























