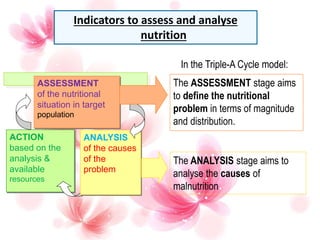
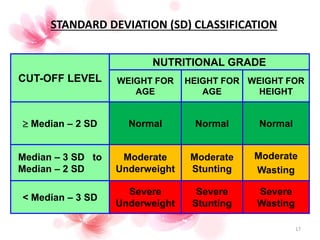
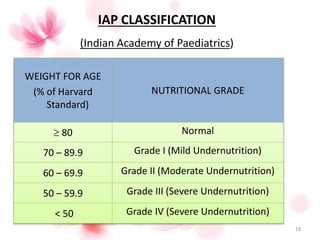
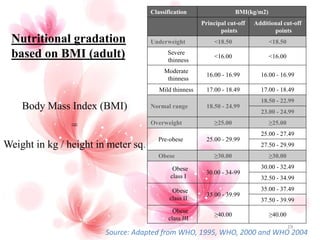
The document discusses the importance of nutritional assessment, specifically focusing on anthropometric measurements, biochemical analysis, clinical evaluation, and dietary assessments. It outlines various methods for evaluating nutritional status, including height, weight, mid-upper arm circumference, and body mass index (BMI). The document also presents classification standards for undernutrition and obesity based on the collected measurements.































































![Assessment of Nutritional Status by Dr.Faryal Shaikh [ August 30th, 2025 ]] f...](https://cdn.slidesharecdn.com/ss_thumbnails/assessmentofnutritionalstatusbydr-251120113500-143fc093-thumbnail.jpg?width=640&height=640&fit=bounds)






































