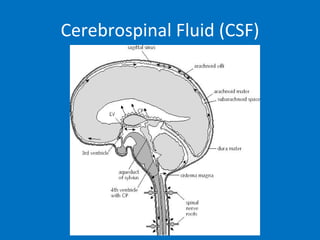
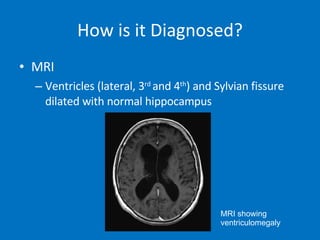
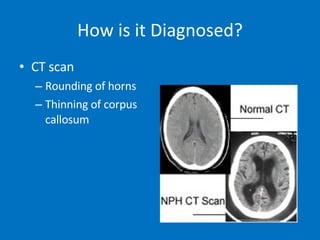
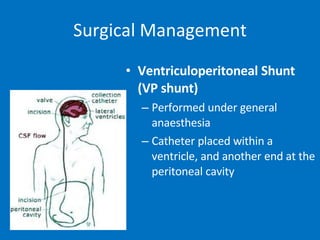
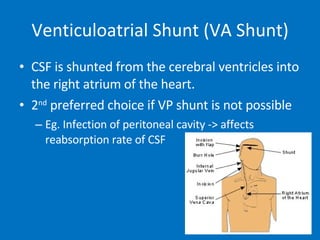
Normal pressure hydrocephalus (NPH) is a condition where cerebrospinal fluid (CSF) absorption is reduced, causing increased pressure in the ventricles of the brain. It typically affects elderly individuals and presents as a triad of symptoms - impaired gait, urinary incontinence, and cognitive impairment. Diagnosis involves MRI or CT scans showing ventricle enlargement. Treatment is usually surgical placement of a shunt to drain CSF from the brain ventricles to the abdominal cavity or heart, which can improve symptoms in many patients. However, shunt surgery also carries risks of complications.












































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


