Introduction
Neonatalemergencies are not uncommon
problems. They appear either at the time of
birth, during the in-hospital post-birth period, or
at home within several weeks of discharge. In
all instances they present significant diagnostic
and treatment challenges to the clinician, and
must be taken seriously.
3.
Definition
Neonate: of, relatingto, or affecting the newborn
and especially the human infant during the first
month after birth
The neonatal period commences at birth and ends
28 completed days after birth.
4.
Etiology - Retrospectiveanalysis of neonatal deaths and stillbirths in
five hospitals in Guyana, December 2007
“This study was conducted in five hospitals:
Georgetown Public Hospital Corporation(GPHC) and
the four Regional Hospitals: New Amsterdam, West
Demerara, Suddie and Linden
McKenzie.”
“These health facilities offer basic and comprehensive
obstetric care to mothers. The results of this study
served to inform the Maternal and Child Health
Department on the issues related to the causative
factors on neonatal deaths and the implications of
service recommendations for the health sector.”
5.
Etiology
The fiveleading causes of neonatal deaths from the
hospitals were:
•Acute respiratory distress,
•Bacterial sepsis of the newborn,
•Birth asphyxia,
•Prematurity and
•Brain haemorrhage: subarachnoid haemorrhage due to the
injuries of the head of the fetus.
Birth injuries to the liver and brain damage occurred in
eleven cases. These issues point to quality of care during
intranatal care.
6.
Mortality Rate
• In2004, the Neonatal Mortality Rate (NMR) was 20.4.
• That is an average of 20.4 children who died not long
after birth for every 1,000 who were born alive.
• This means that at least 334 of the children recorded in
16,391 live birth figures for 2004 are not alive today.
• In 2000, NMR = 54.0
• In 2006, NMR = 37.0
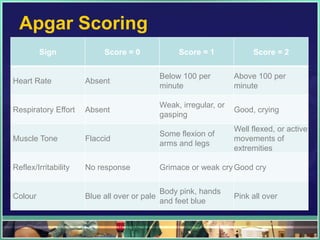
Apgar Scoring
Sign Score = 0 Score = 1 Score = 2
Below 100 per Above 100 per
Heart Rate Absent
minute minute
Weak, irregular, or
Respiratory Effort Absent Good, crying
gasping
Well flexed, or active
Some flexion of
Muscle Tone Flaccid movements of
arms and legs
extremities
Reflex/Irritability No response Grimace or weak cry Good cry
Body pink, hands
Colour Blue all over or pale Pink all over
and feet blue
Signs & symptoms
•The clinical symptoms may be nonspecific.
• The history may reveal only a change in
feeding pattern or subtle behavioral changes.
12.
Differential Diagnosis
• Auseful mnemonic to recall the broad differential diagnosis
of a neonate with altered mental status:
‘‘THE MISFITS’’
13.
THE MISFITS
T-Trauma (non-accidental and accidental)
H-Heart disease/Hypovolemia/Hypoxia
E-Endocrine (congenital adrenal
hyperplasia, thyrotoxicosis)
M-Metabolic (electrolyte imbalance)
I-Inborn errors of metabolism (metabolic emergencies)
S-Sepsis (meningitis, pneumonia, urinary tract infection)
F-Formula mishaps (under or over dilution)
I-Intestinal conditions
(volvulus, intussusception, necrotizing enterocolitis)
T-Toxins/Poisons
S-Seizures
14.
Trauma
• Classified asAccidental or Non-accidental
• Non-accidental head trauma may only have subtle
historical findings and no physical exam findings
• Presenting symptoms may be nonspecific
• Early diagnosis of an occult head injury may
prevent significant long-term morbidity
15.
Trauma -Accidental
• Mosthead injuries occur secondary to motor vehicle
accidents, falls, assaults, recreational activities, and child
abuse.
• Mechanical or anoxic trauma incurred by the neonate during
labor or delivery include:
• Head and scalp injuries
• Cephalhematoma
• Subgaleal Hematoma
• Caput Succedameum
• Vacuum Caput
16.
Trauma- Accidental
OrthopedicInjuries and Fractures
Clavile Fracture from Birth Trauma
Skull Fracture from Birth Trauma
Sternocleidomastoid Hematoma (Torticollis)
Peripheral Nerve Injuries
Facial Nerve Injury from Birth Trauma
Brachial Plexus from Birth Trauma
Duchenne-Erb Paralysis
Klumpke‟s Paralysis
Phrenic Nerve Injury from Birth Trauma
Recurrent Laryngeal Nerve Injury from trauma
17.
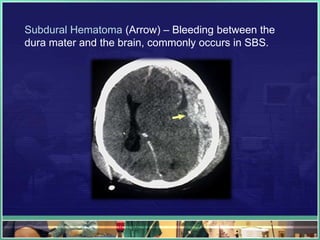
Shaken Baby Syndrome-Nonaccidental
•Shaken baby syndrome is a severe form of child abuse
caused by violently shaking an infant or child.
• The brain bounces back and forth against the skull.
• Causes bruising of the brain (cerebral contusion),
swelling, pressure, and bleeding in the brain.
• The large veins along the outside of the brain may tear,
leading to further bleeding, swelling, and increased
pressure.
• This can easily cause permanent brain damage or death.
Signs & Symptoms
Varyfrom mild to severe:
• Convulsions (seizures)
• Decreased alertness
• Extreme irritability or other changes in behavior
• Lethargy, sleepiness, not smiling
• Loss of consciousness
• Loss of vision
• No breathing
• Pale or bluish skin
• Poor feeding, lack of appetite
• Vomiting
20.
Treatment
Treatment involves:
• Monitoringof intracranial pressure (the pressure
within the skull),
• Draining of fluid from the cerebral ventricles,
• Draining of intracranial hematoma if present.
Prevention
•NEVER shakea baby or child in play or in anger. Even gentle
shaking can become violent shaking when you are angry.
•Do not hold your baby during an argument.
•If you find yourself becoming annoyed or angry with your
baby, put him in the crib and leave the room. Try to calm down.
Call someone for support.
•Call a friend or relative to come and stay with the child if you feel
out of control.
•Contact a local crisis hotline or child abuse hotline for help and
guidance.
•Seek the help of a counselor and attend parenting classes.
•Do not ignore the signs if you suspect child abuse in your home
or in the home of someone you know.
23.
Heart Disease
• Congenitalheart diseases (CHD) encompass a
spectrum of structural abnormalities of the heart or
intra-thoracic vessels.
• Commonly presents in the newborn with central
cyanosis, heart failure, sudden collapse or heart
murmur.
• Classified as Cyanotic or Acyanotic
24.
Cyanotic Heart Disease
•Cyanosis is a pathologic process caused by
deoxygenated blood in the capillary vessels.
• Cyanotic heart defects are not detected in the
newborn nursery, presents during the first 2 to 3
weeks of life when the Ductus Arteriosus closes .
• There is still adequate oxygenated blood to the
systemic circulation through a patent DA.
25.
Terrible T‟s
The congenitalheart defects that classically present
with cyanosis, commonly referred to as the „„Terrible
Ts”
1. Transposition of the great vessels
2. Total anomalous pulmonary venous return
3. Tetralogy of Fallot
4. Truncus arteriosus
5. Tricuspid atresia
26.
Acyanotic Heart Disease
•Acyanotic heart diseases may also be a result of closure of
the ductus arteriosus (DA).
• The onset of symptoms typically is gradual, with the onset of
congestive heart failure.
• Different degrees of obstruction to the left ventricular outflow
tract are present that result in an increase in pulmonary
blood flow and a gradual development of heart failure.
27.
Signs & Symptoms
•Tachypnea
•Tachycardia
•Hepatomegaly
•History of poor feeding
•Sweating or color change with feedings
•Poor weight gain
• Lower extremity edema and jugular venous
distention are unlikely findings at this age
28.
Common Causes
•Anemia •Endocardial cushion defect
•Aortic atresia •Hypoplastic left heart
•Aortic stenosis •Interrupted aortic arch
•Arteriovenous malformation •Mitral valve atresia
•Coarctation of the Aorta •Patent ductus arteriosus
•Complete arteriovenous •Truncus arteriosus
canal
•Cor pulmonale caused by •Ventricular septal defect
bronchopulmonary dysplasia
29.
Management - ClassicHyperoxia Test
•Differentiate between cardiac and noncardiac causes
•Provide 100% oxygen
•Observe the oxygen saturation on pulse oximetry for
an increase of 10% in pulmonary causes (PaO2
should increase by 30 mm Hg)
•If the neonate‟s oxygen saturation or PaO2 fail to
improve, cyanotic heart disease is suspected.
30.
Management
• Administration ofprostaglandin E1 (PGE1) as a bolus of
0.05 mcg/kg IV
• Success is less likely because the development of heart
failure is gradual and the DA may already have been closed
for several days to weeks.
• First line -Furosemide, 1 mg/kg IV
Other adjuvants include dopamine, dobutamine, and digoxin.
• Pediatric cardiology consultation
31.
Endocrine
• Congenital adrenalhyperplasia - Congenital
adrenal hyperplasia refers to a group of inherited
disorders of the adrenal gland.
• Thyrotoxicosis (Hyperthyroidism) - Thyroid gland
makes too much thyroid hormone. The condition is
often referred to as an "overactive thyroid."
32.
Congenital adrenal hyperplasia
Causedby a deficiency in the 21-hydroxylase
enzyme - needed for biosynthesis of the steroid
hormones aldosterone and cortisol.
Patient may present in the first few weeks of life with
symptoms:
•Vomiting
• hypoglycemia
• or even shock.
33.
Thyrotoxicosis
Infants born tomothers with Graves‟ disease may develop
thyrotoxicosis and present with delayed symptoms to the ED.
Symptoms may include:
•Poor feeding, irritability, tachycardia, respiratory distress,
hyperthermia, or congestive heart failure.
Treatment:
•Propranolol,0.25 mg/kg IV- to control tachycardia.
•In addition, propylthiouracil, 1.25 mg/kg IV,
•followed by Lugol‟s solution (1–5 drops orally)- to control the
hypermetabolic state and hormone release
34.
Metabolic
• Genetic disordersin which the body cannot
properly turn food into energy.
• Usually caused by defects in specific proteins
(enzymes) that help break down (metabolize) parts
of food.
• Problems arise due to accumulation of substances
which are toxic or interfere with normal function.
35.
Inborn Errors ofmetabolism
• Nonspecific symptoms: poor feeding, vomiting,
failure to thrive, tachycardia, tachypnea, or
irritability.
• Occasionally the diagnosis may be more apparent
and include symptoms of seizures, lethargy,
hypoglycemia, apnea, temperature instability, and
acidosis.
• Physical exam findings are usually normal.
Sepsis
• Neonatal sepsisis a blood infection that occurs in
an infant younger than 90 days old.
• Early-onset sepsis is seen in the first week of life.
• Late-onset sepsis occurs between days 8 and 89.
38.
Causes
A number ofdifferent bacteria, including :
• Escherichia coli ( E. coli),
• Listeria
• Certain strains of streptococcus
• Early-onset neonatal sepsis-appears within 24
hours of birth.
39.
Causes
The following increasesan infant's risk of early-onset
sepsis:
•Group B streptococcus infection during pregnancy
•Preterm delivery
•Water breaking (rupture of membranes) that lasts
longer than 24 hours before birth
•Infection of the placenta tissues and amniotic fluid
(chorioamnionitis)
40.
Signs & Symptoms
•Bodytemperature changes
•Breathing problems
•Diarrhea
•Low blood sugar
•Reduced movements
•Reduced sucking
•Seizures
•Slow heart rate
•Swollen belly area
•Vomiting
•Yellow skin and whites of the eyes (jaundice)
41.
Treatment
Recommended Antibiotics andDosages for Neonatal
Sepsis:
• Ampicillin 50-100 mg/kg IV
• Gentamicin 2 mg/kg IV
• Cefotaxime 50-100 mg/kg IV
• Acyclovir 20 mg/kg IV
Formula Mishaps
• Theinappropriate mixing of water, powdered
formula or overdilution of concentrated liquid or
premixed formula may result in life-threatening
electrolyte disturbances or failure to thrive.
• Hyponatremia may present as seizures and
requires recognition of an electrolyte abnormality
and immediate correction to stop the seizure
Toxins/ Poisons
• Toxicingestions are uncommon in this age group,
but occasionally result from a maternal ingestion in
a breastfeeding mother, homeopathic remedies, or
overuse of accepted medications.
46.
Seizures
•Seizures occurring duringthe neonatal period are
often difficult to recognize.
•The cortical development is not complete, and as a
result, generalized motor activity is less common.
•Subtle seizures in the term neonate can include
abnormal eye movements (usually
horizontal, sustained eye deviation), lip
smacking, abnormal
tongue movements, pedaling, or apnea.
47.
Classifications
Clonic seizures
These movementsmost commonly are associated
with electrographic seizures.
They often involve 1 extremity or 1 side of the body.
The rhythm of the clonic movements is usually
slow, at 1-3 movements per second.
48.
Classification
•Tonic seizures
•These mayinvolve 1 extremity or the whole body. Focal tonic
seizures involving 1 extremity often are associated with
electrographic seizures.
•Generalized tonic seizures often manifest with tonic extension
of the upper and lower limbs and also may involve the axial
musculature in an opisthotonic fashion.
•Generalized tonic seizures mimic decorticate posturing; the
majority are not associated with electrographic seizures.
49.
Classification
Myoclonic seizures
•These mayoccur focally in 1 extremity or in several
body parts (in which case they are described as
multifocal myoclonic seizures).
•Focal and multifocal myoclonic seizures typically are
not associated with electrographic correlates.
•Generalized myoclonic jerks are possibly the clinical
equivalent of infantile spasms.
50.
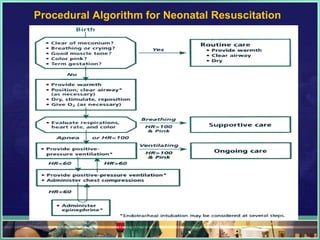
Acute Management ofNeonatal Seizures
After each step, evaluate the infant for ongoing seizures. If seizures persist,
advance to next step
Step 1. Stabilize vital functions
Step 2. Correct transient metabolic disturbances
A. Hypoglycemia (target blood sugar 70-120 mg/dL)
10% dextrose water IV bolus dose 2 mL/kg followed by a continuous
infusion at 8 mg/kg/min
B. Hypocalcemia 5% calcium gluconate IV at 4 mL/kg (need cardiac
monitoring)
C. Hypomagnesemia 50% magnesium sulfate IM at 0.2 mL/kg
51.
Acute Management ofNeonatal Seizures
Step 3. Phenobarbital 20 mg/kg IV load
Cardiorespiratory monitoring
5 mg/kg IV (may repeat to total dose of 40 mg/kg)
Consider continuous EEG monitoring
Consider intubation/ventilation
Step 4. Lorazepam 0.05 mg/kg IV (may repeat to
total dose of 0.1 mg/kg)
52.
Acute Management ofNeonatal Seizures
Step 5. Phenytoin (fosphenytoin)
20 mg/kg slow IV load
5 mg/kg slow IV (may repeat to total dose of 30
mg/kg)
Step 6. Pyridoxine 50-100 mg/kg IV (with *EEG
monitoring)
*EEG = electroencephalogram.
Recommendations-Postnatal and NewBorn care
Essential newborn care for all newborns should ensure:
• Birth in a safe environment with access to complete obstetric and neonatal care.
• Avoid unjustified separation from the mother.
• Early and exclusive breastfeeding: early suckling, positioning and attaching the
baby to the breast; rooming-in and unrestricted feeding; ten steps to successful
breastfeeding; safe human milk banking.
• Warmth provision and avoidance of bathing during first 24 hours.
• Infection control, including cord care and hygiene.
• Postpartum vitamin A provided to mother.
• Eye prophylaxis to prevent gonococcal opthalmia.
• Information and counseling for home care and emergency preparedness.
56.
Recommendations
Extra care forsmall babies
• Extra home visits; support for breastfeeding, thermal care, and hygienic
cord care.
• Extra attention to warmth, feeding support, and early identification and
management of complications.
• Skin to skin thermal care (kangaroo mother care).
• Vitamin K administration at birth.
• Facility-based clinical care of ill newborn babies, particularly those with
infections, prematurity, and birth asphyxia. Short and long term follow up.
• Early neurodevelopment stimulation.
57.
Recommendations
Pre-discharge package (atfacility level or before birth attendant leaves the
mother in the case of a home delivery)
• Careful assessment of high risk factors/danger signs (for both mother and
newborn).
• Counseling for mother and family in preventive care, recognition of danger signs,
provision of care (what to do and where to go).
• Promotion and referral for early postnatal care.
• Follow-up care for birth spacing, immunization, nutrition (breastfeeding), growth
monitoring and development of baby.
58.
Recommendations
Assure appropriate carein the home for the mother and newborn
• Effective empowerment, participation and communication strategies
including community involvement in planning MNCH programs.
• Community mobilization and engagement, and antenatal and post natal
domiciliary behaviour change communications to promote:
1. evidence-based care practices (breastfeeding, thermal care, and clean
cord care),
2. care seeking, and
3. demand for quality clinical care.
59.
References
•Merriam-Webster‟s Learner‟s Dictionary
http://www.learnersdictionary.com/search/neonatal
•TheMaternal and Child Health Department
Ministry of Health, Brickdam, Georgetown
Retrospective analysis of neonatal deaths and stillbirths in five hospitals in
Guyana,December 2007
•Bureau of Statistics
57 High Street, Kingston, Georgetown - Multiple Indicator Cluster Survey
Summary Report 2006
http://www.statisticsguyana.gov.gy/pubs/Guyana_MICS_Summary_Report
_2006.pdf
Editor's Notes
#14 A classic pneumonic used by Neonatologists and Pediatric Emergency Physicians.