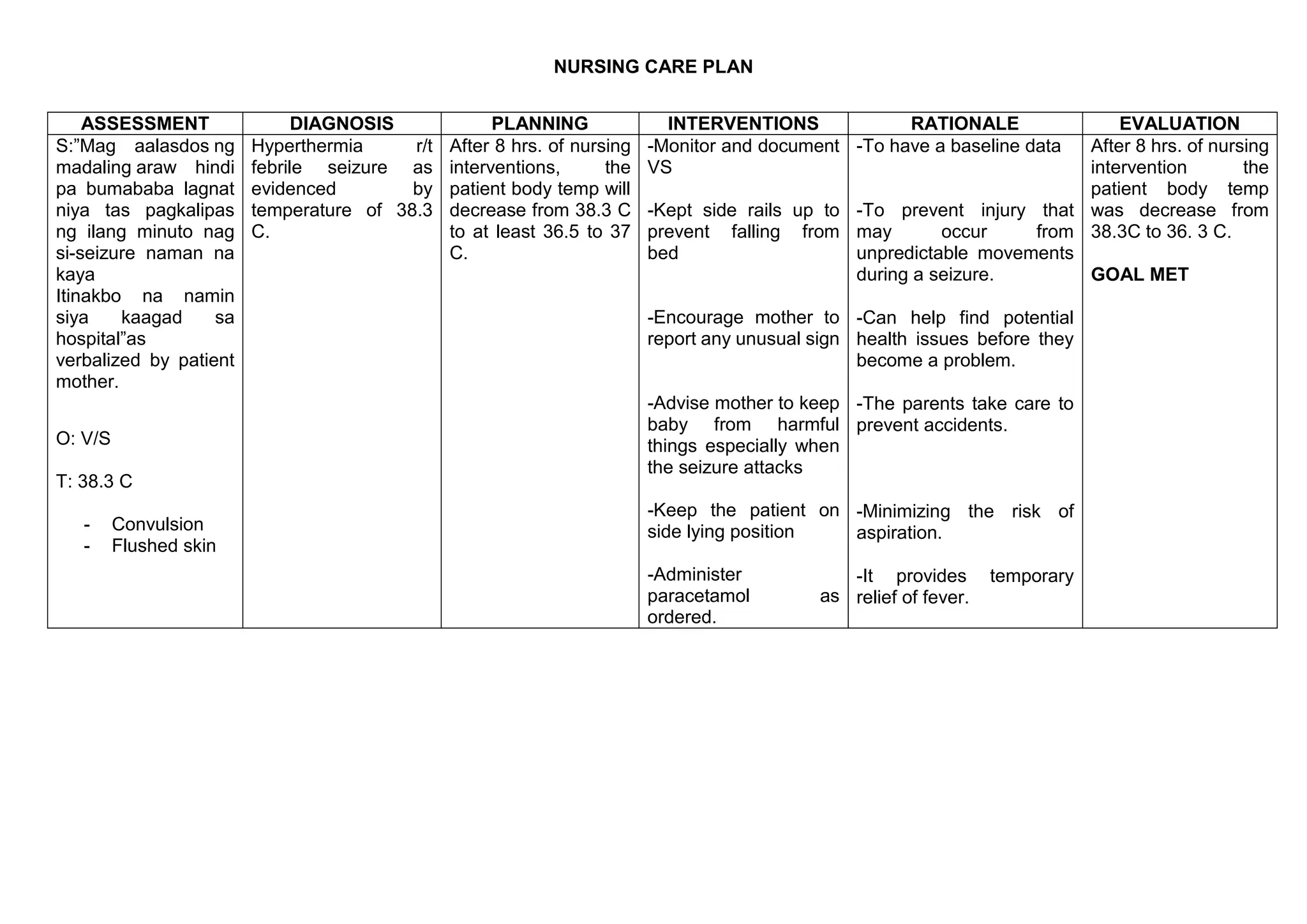
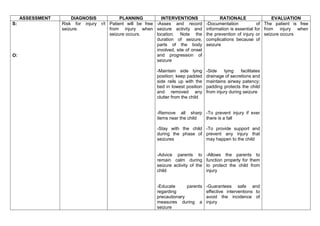
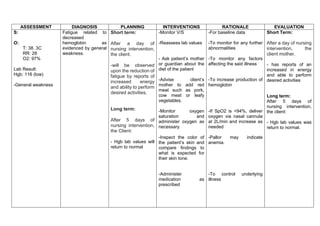
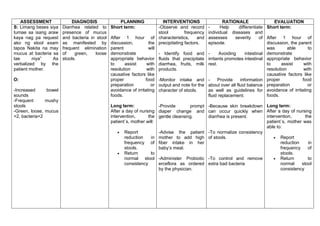
The document outlines a nursing care plan that includes assessments, diagnoses, planning, interventions, rationales, and evaluations for a pediatric patient presenting with febrile seizures, anemia, diarrhea, and risk for impaired mobility. It details specific nursing interventions aimed at stabilizing the patient's condition and preventing complications, including monitoring vital signs, managing symptoms, and educating the parents on care strategies. The evaluation indicates that after 8 hours to 5 days of interventions, the patient shows improvement in temperature, hemoglobin levels, stool consistency, and comfort from pain.