Download as PDF, PPTX



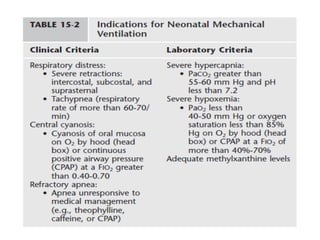
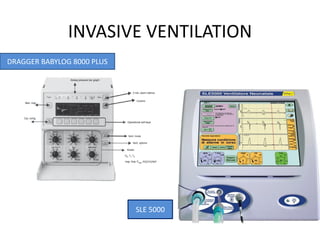
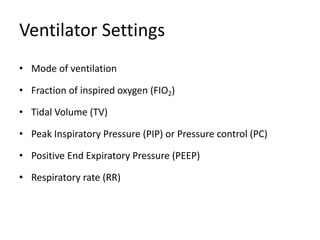


The document discusses the basics of neonatal ventilation, covering indications, settings, techniques, complications, and weaning strategies. It highlights two main approaches: non-invasive and invasive ventilation, detailing specific methods such as CPAP and high-frequency ventilation, along with troubleshooting and complications associated with mechanical ventilation. Additionally, it emphasizes the importance of careful weaning and the potential risks of mechanical ventilation in neonates, underlining the need for optimal ventilation practices.































































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)



