Download to read offline
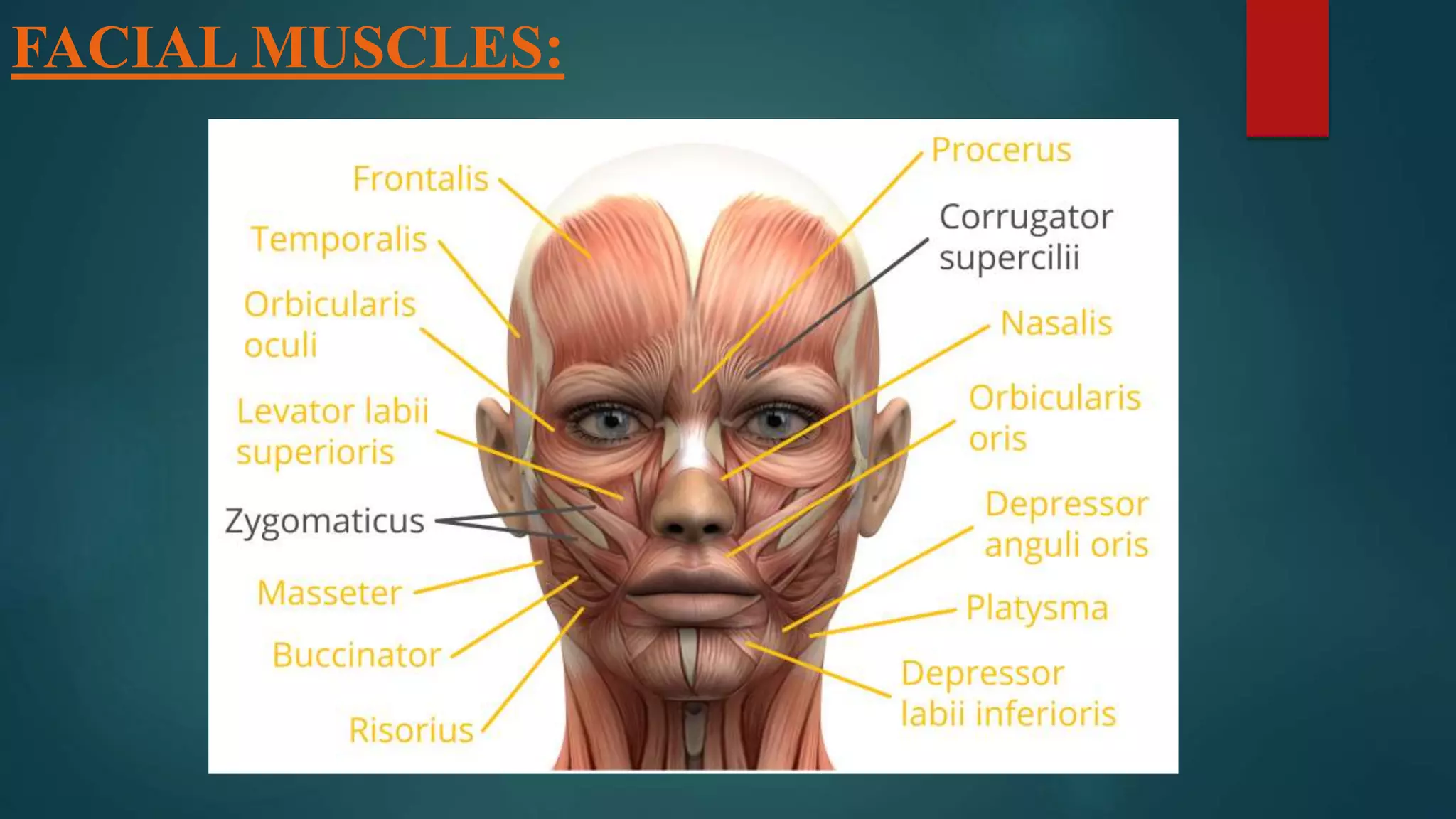
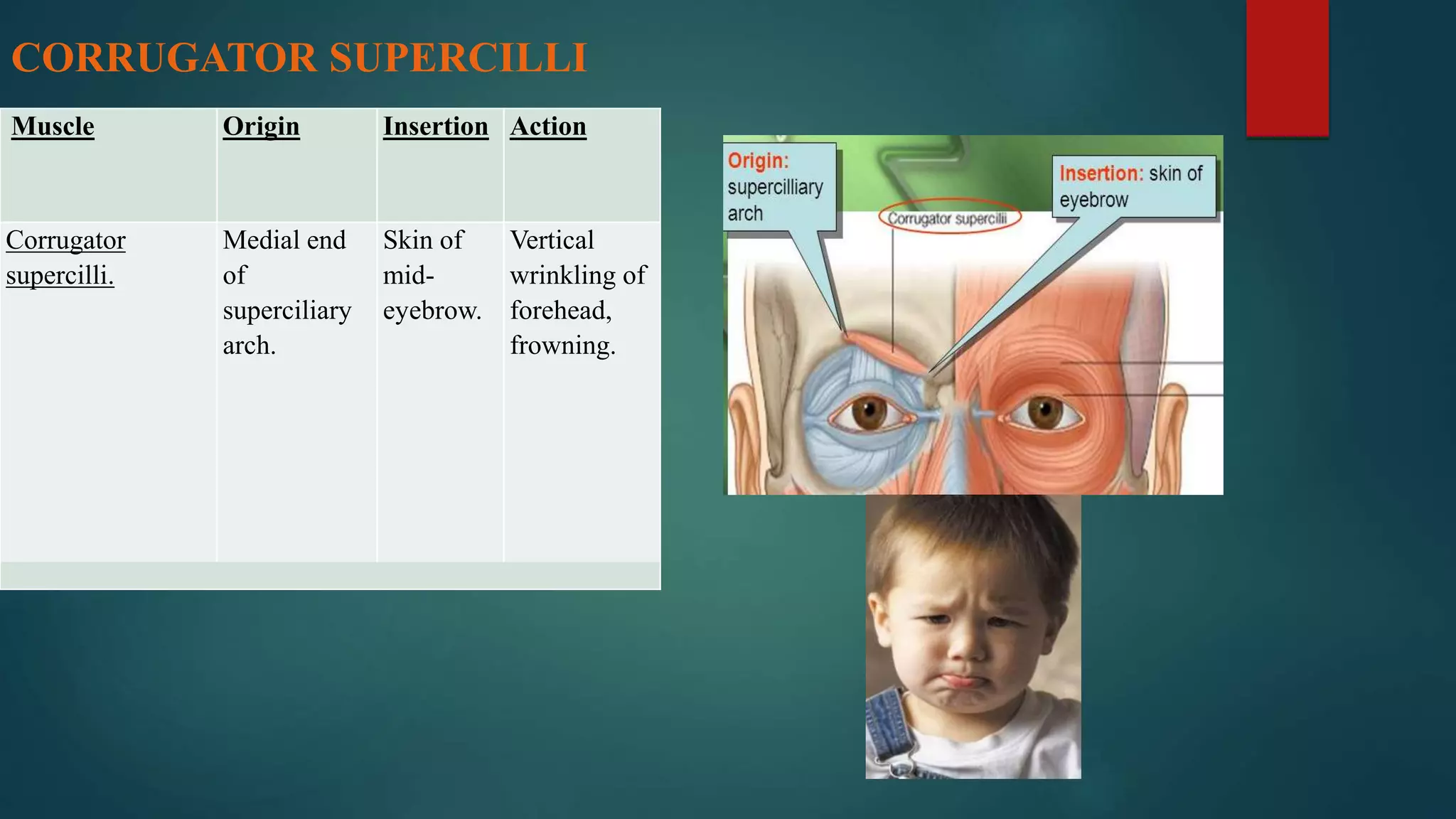
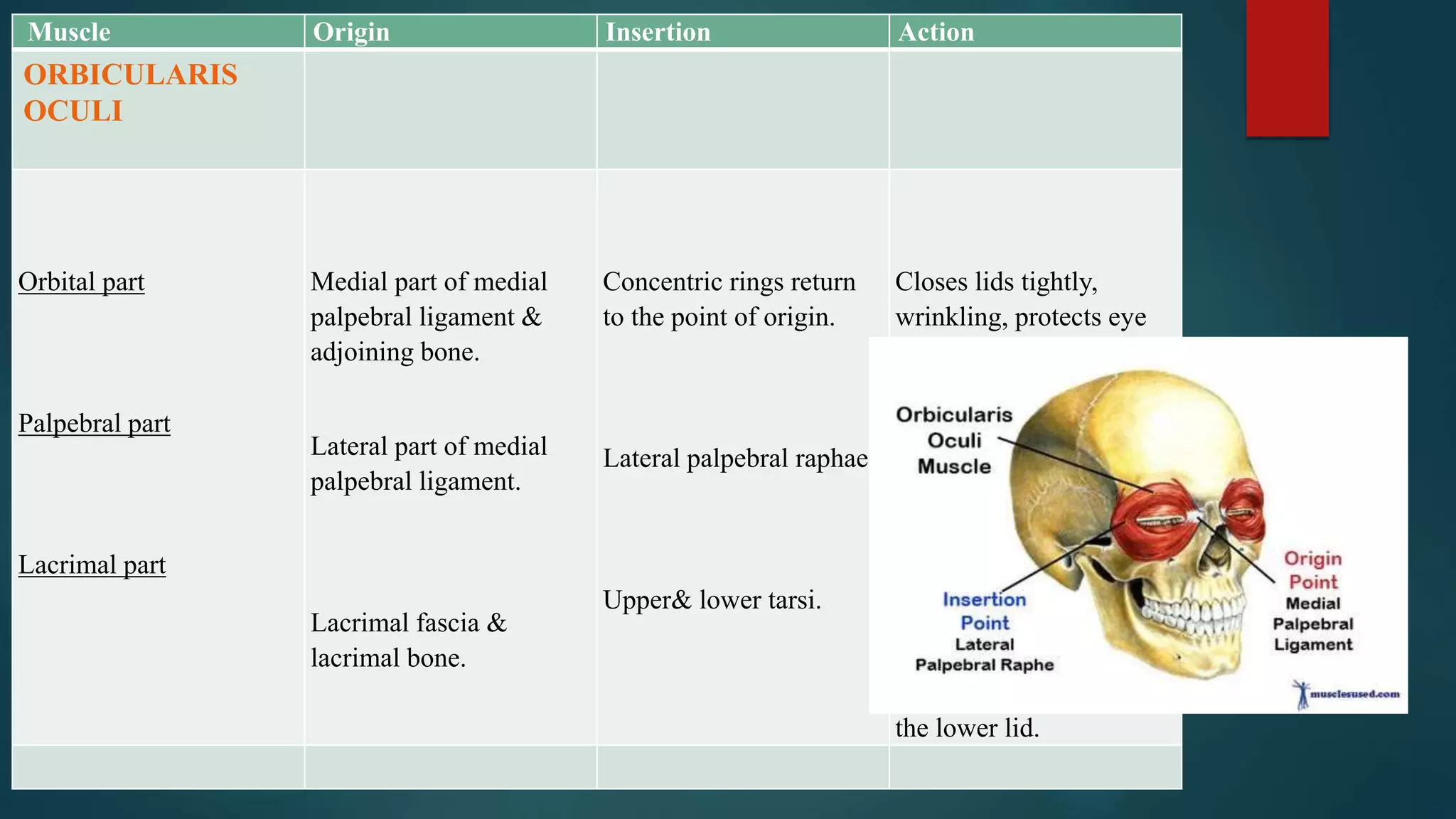
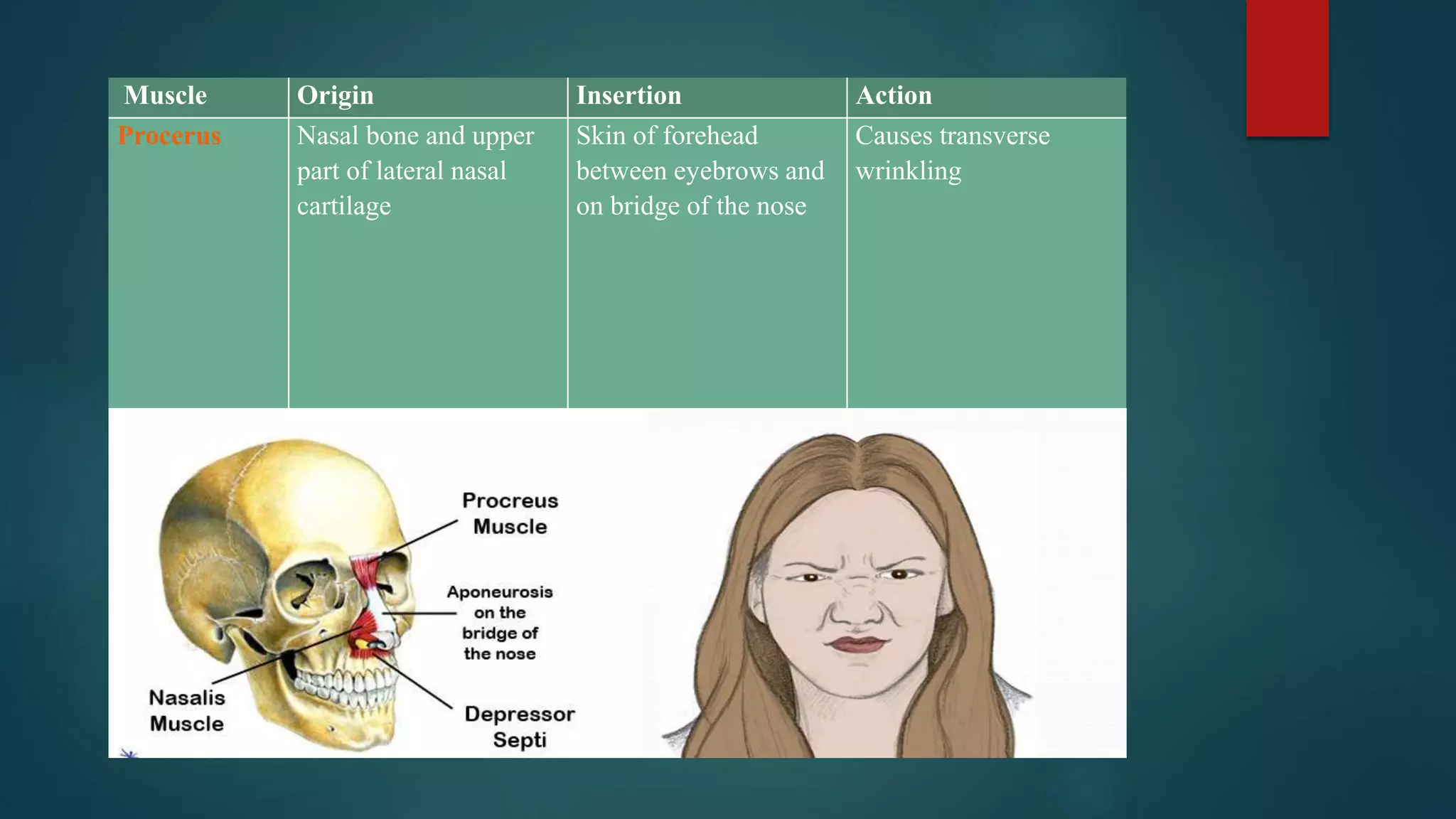

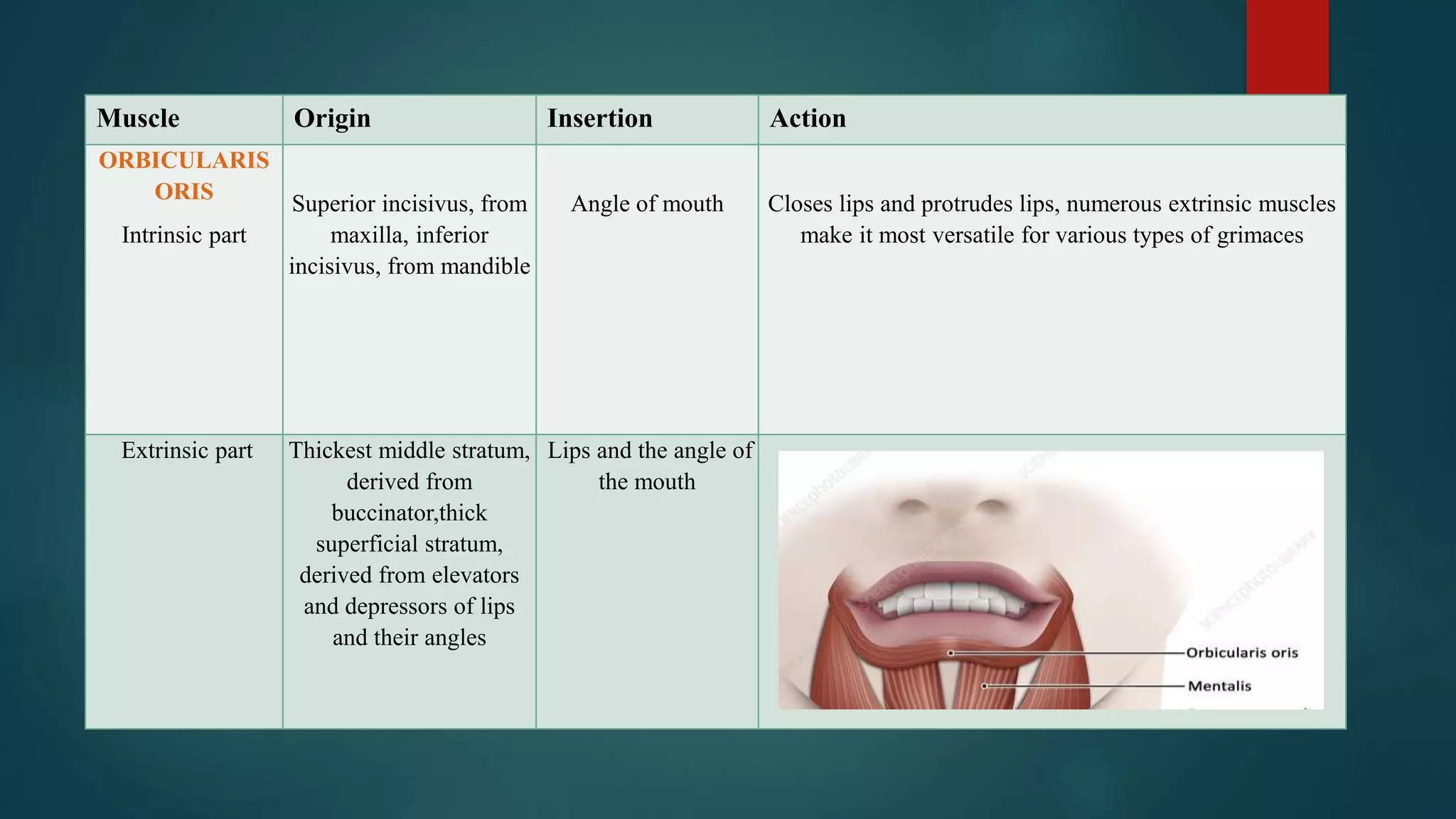
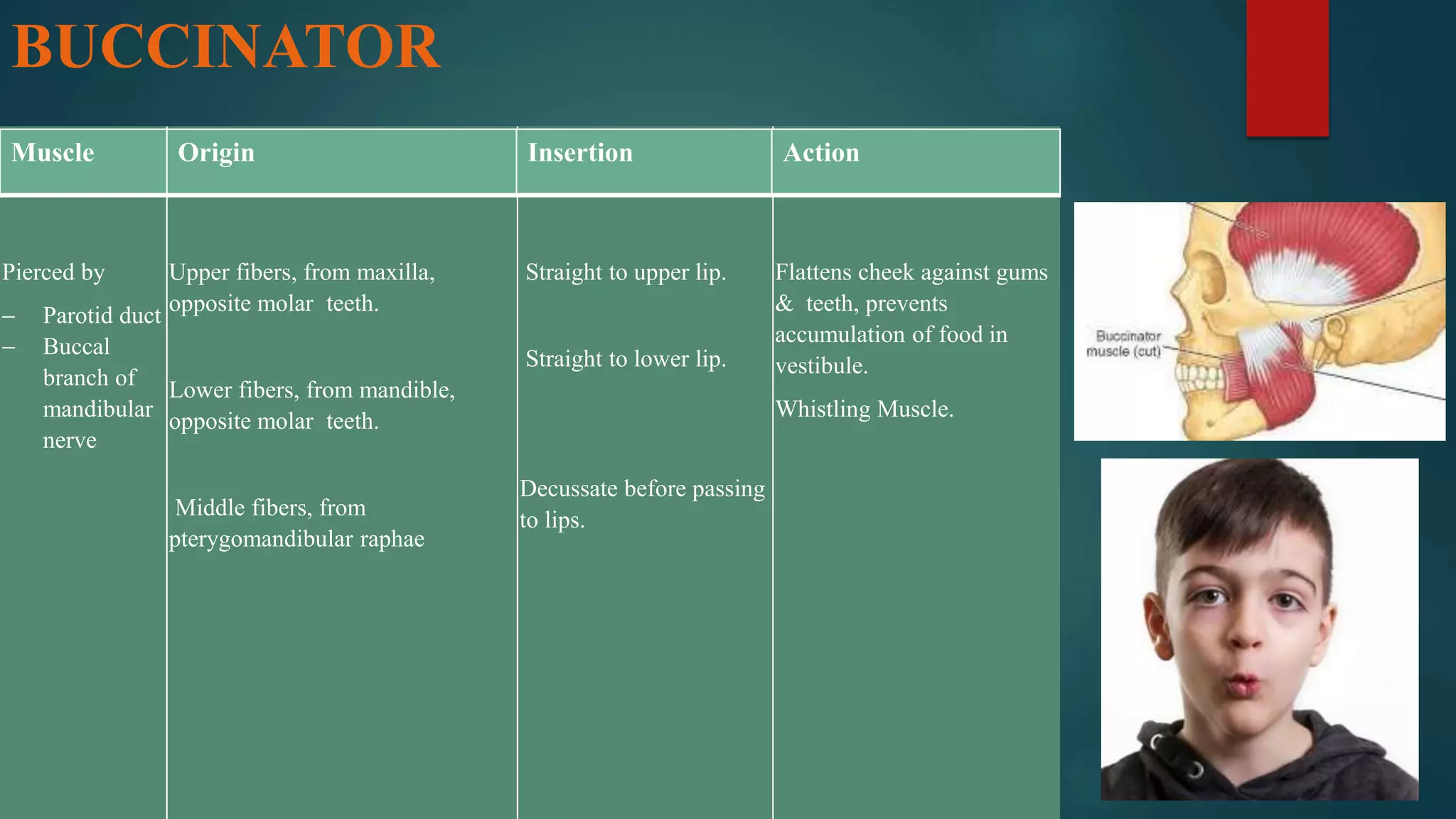
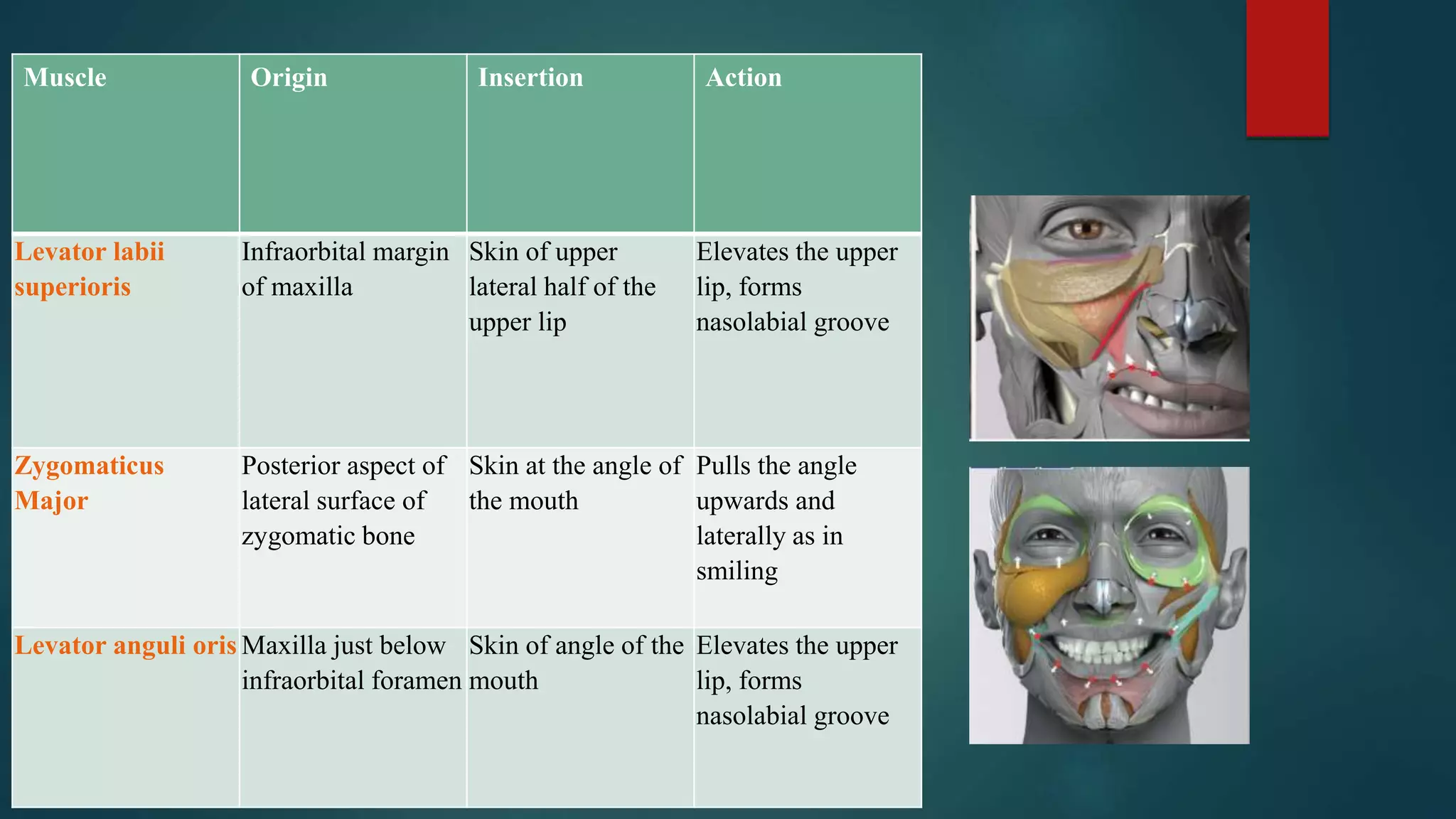
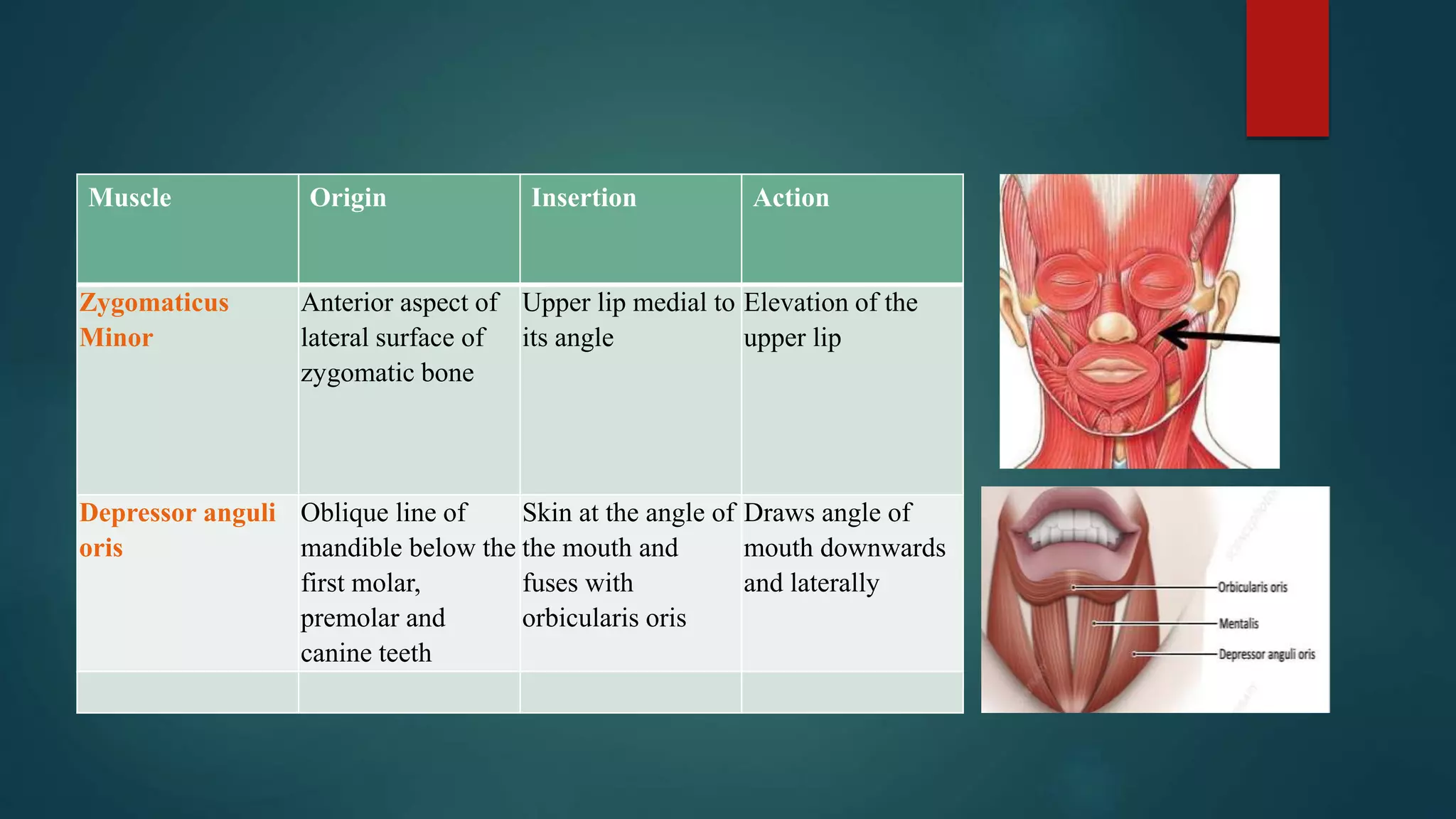
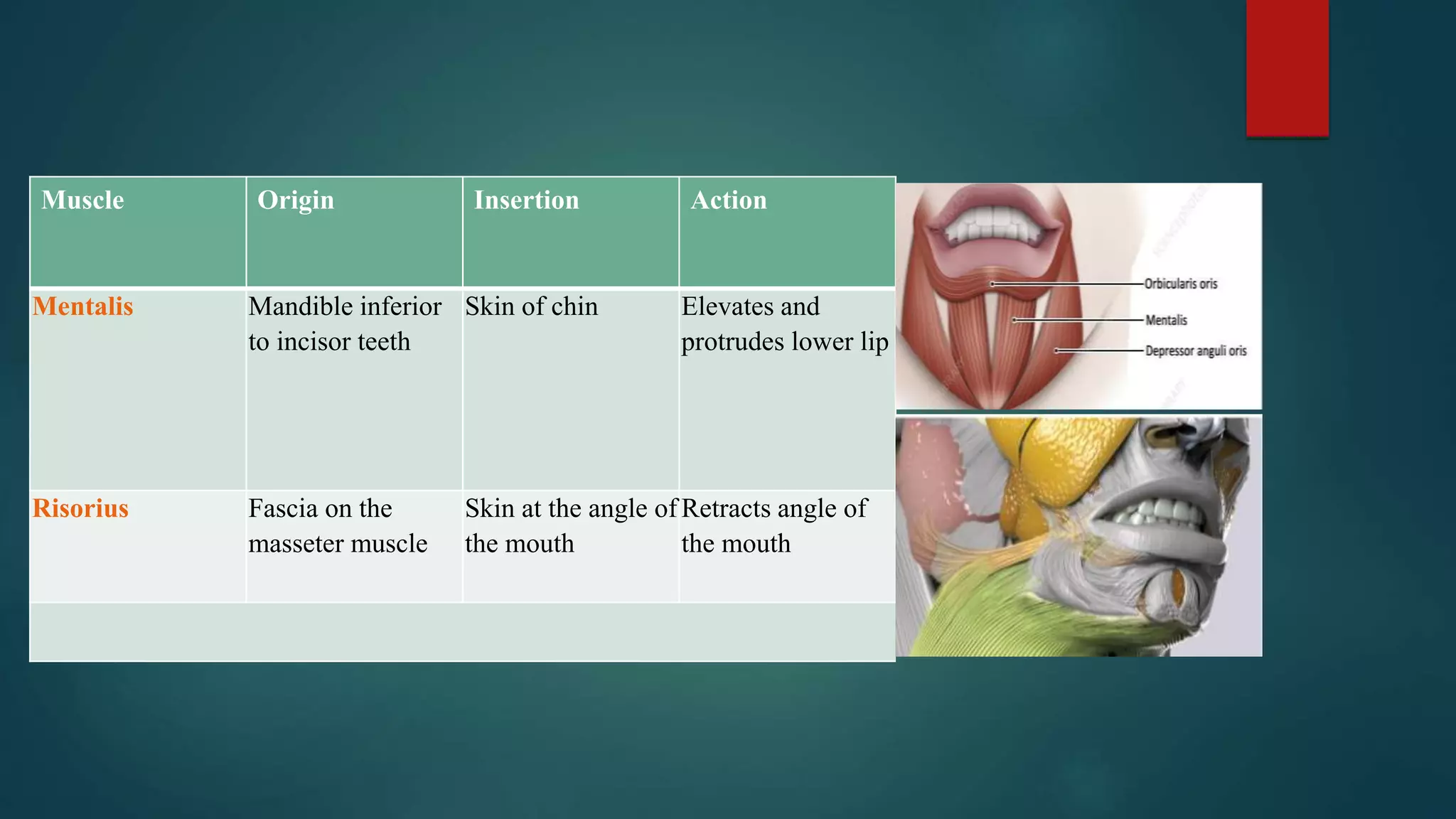
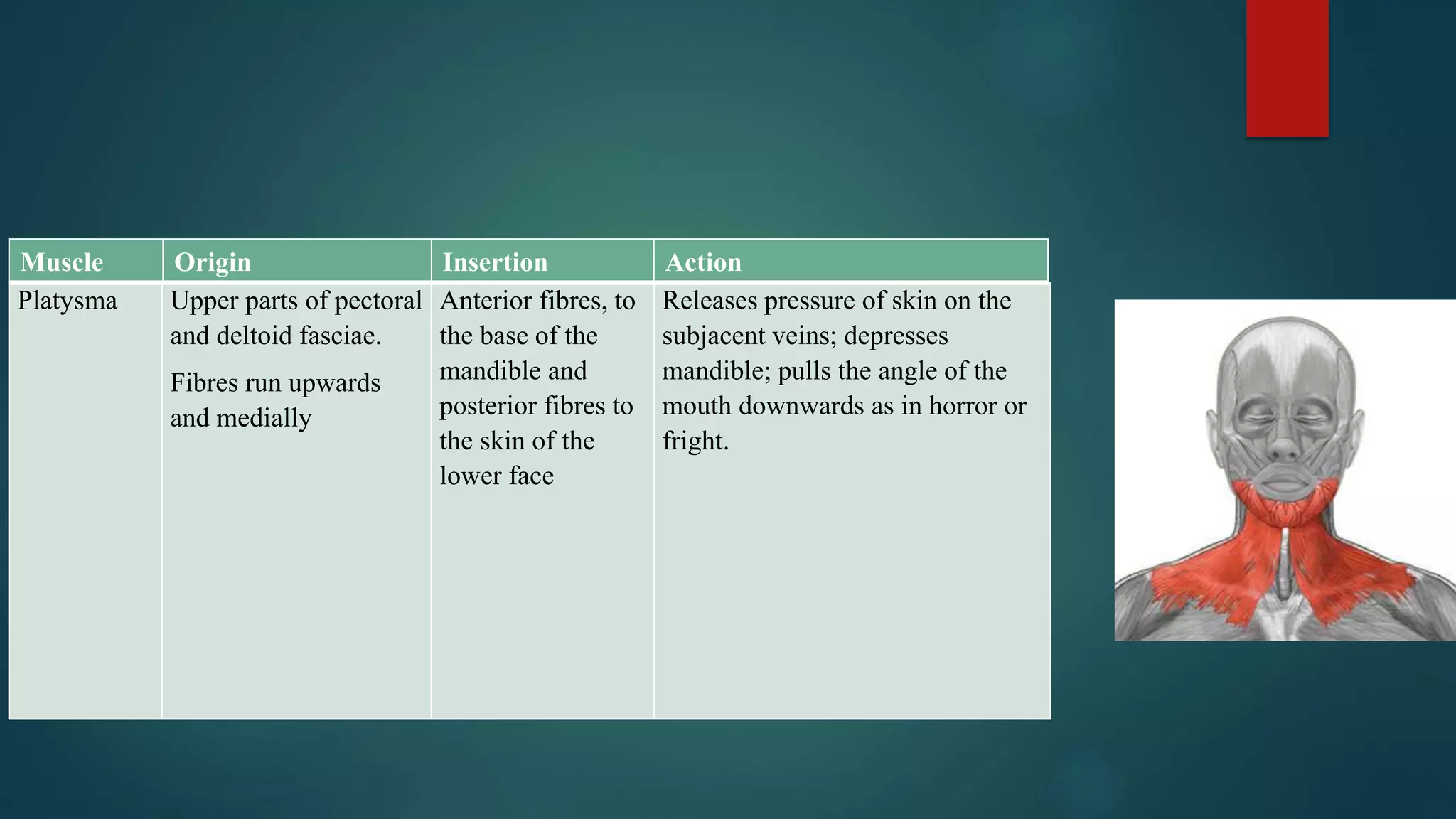

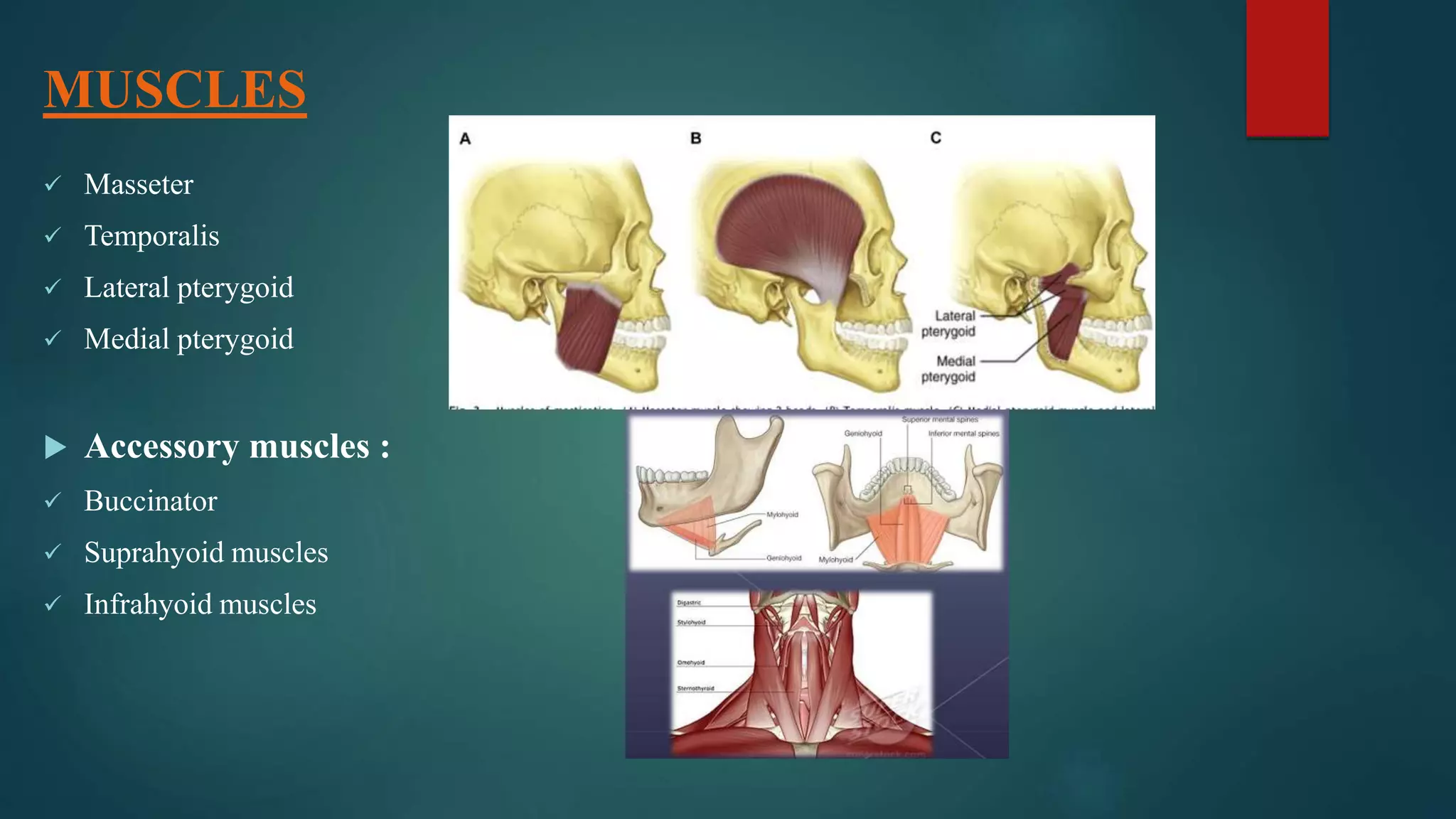
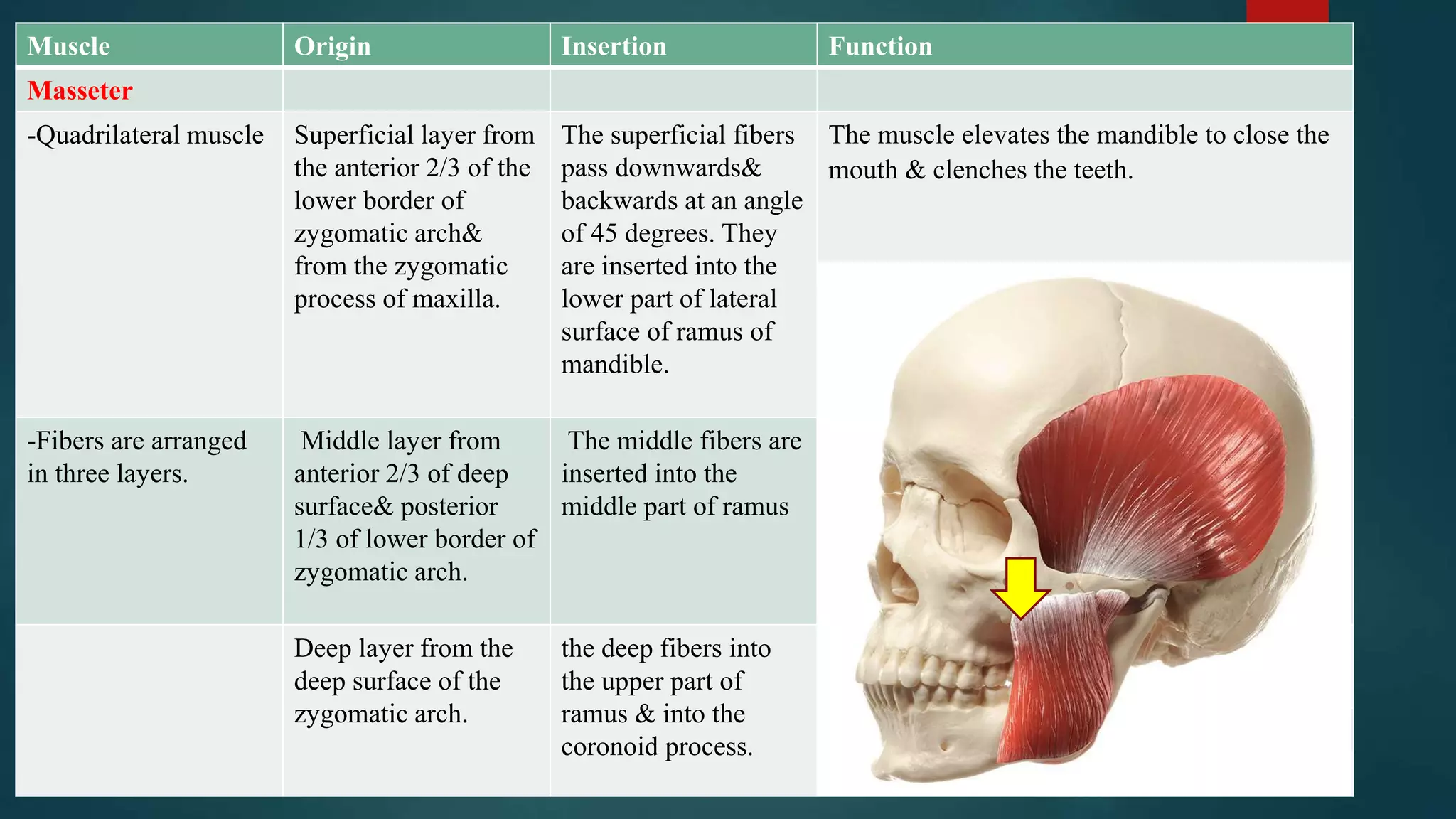
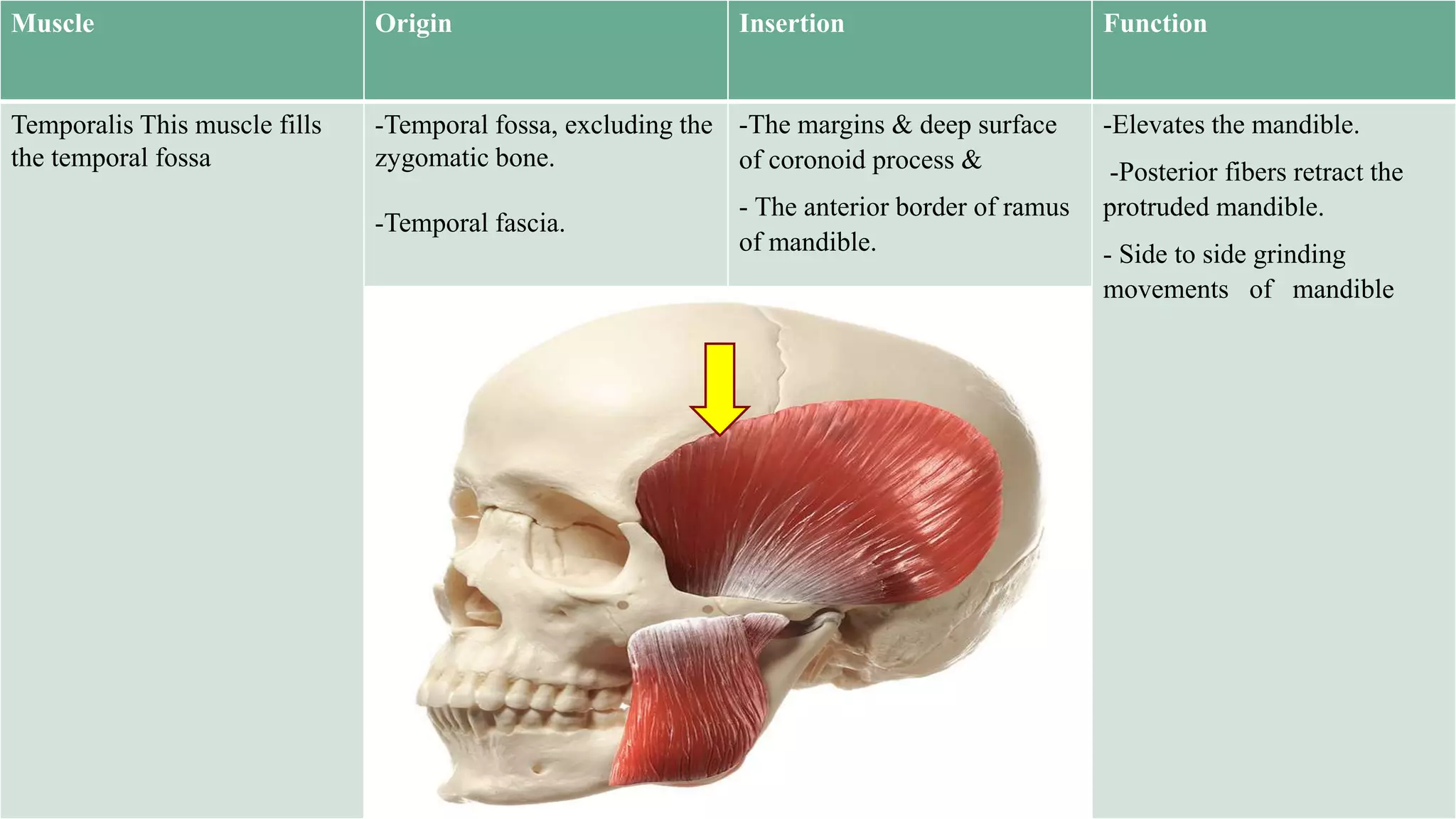
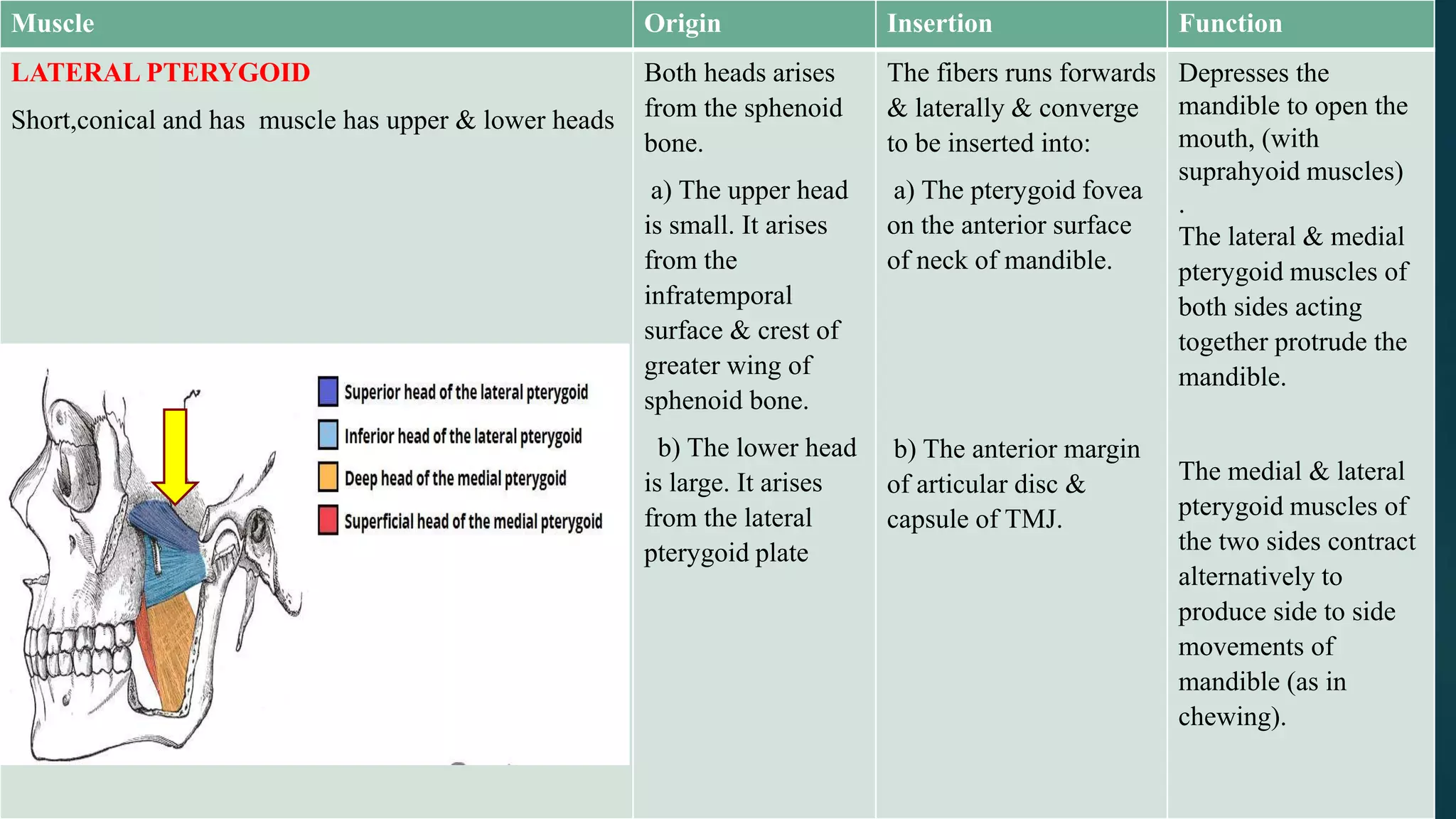
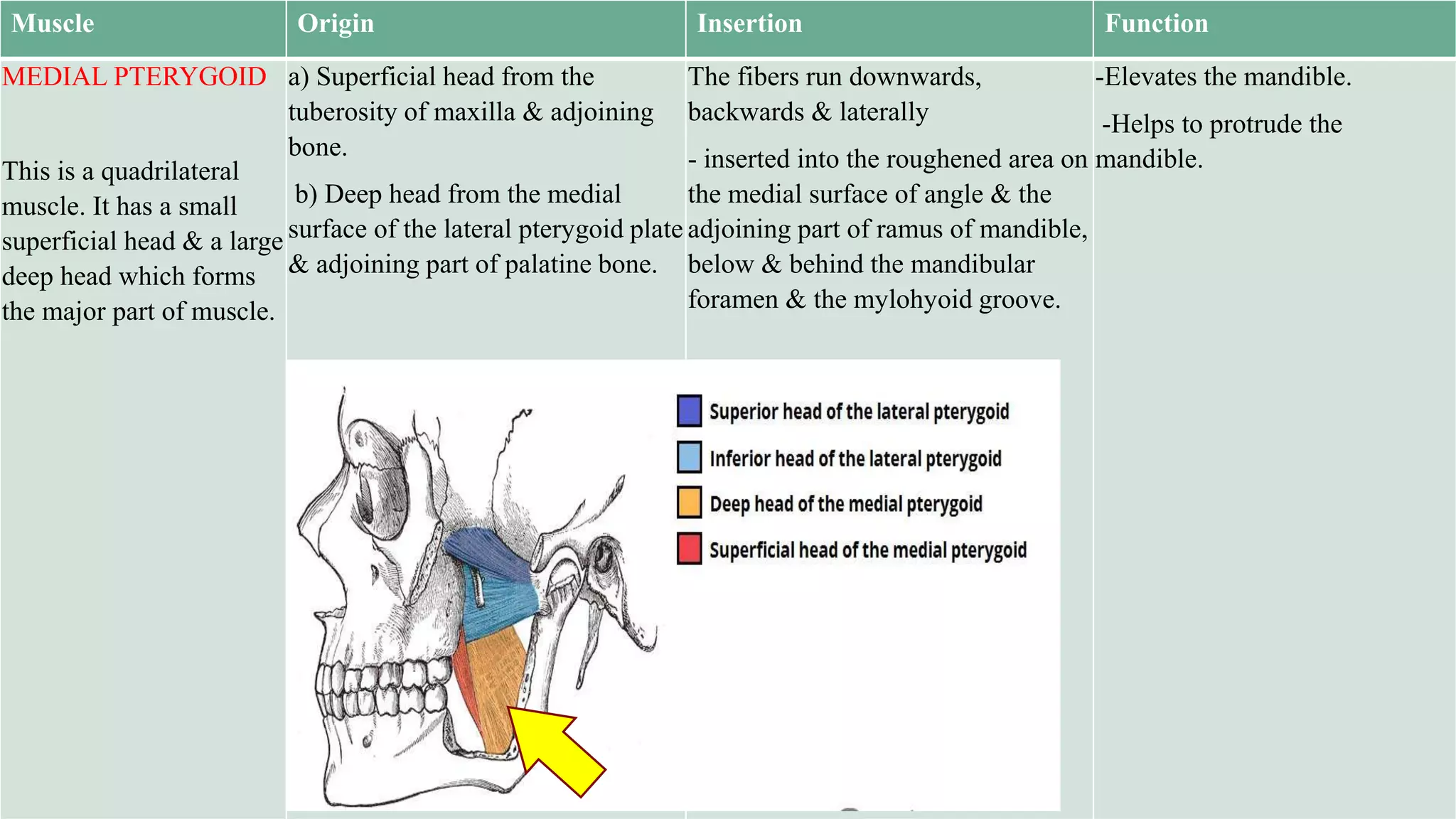
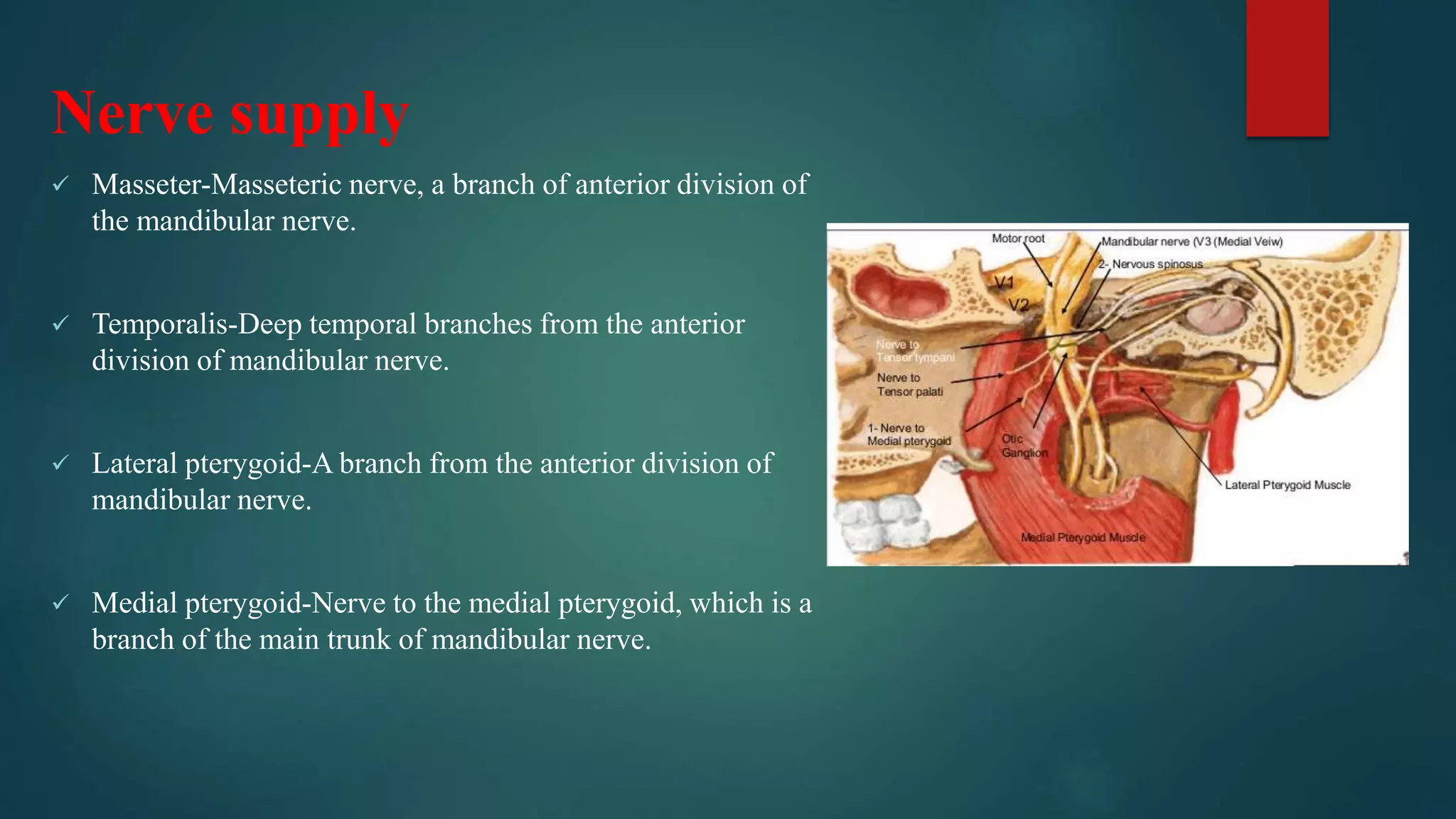
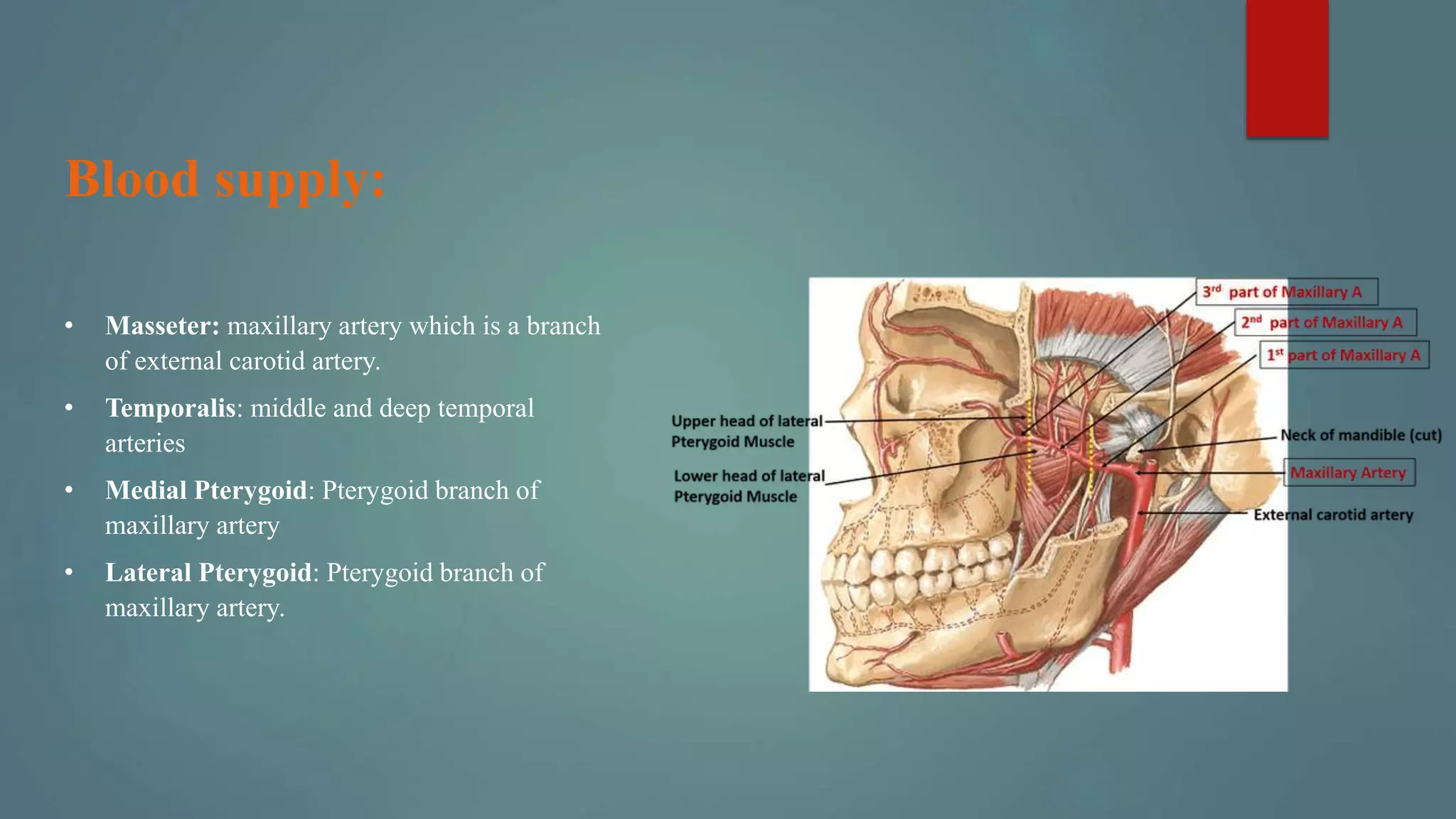
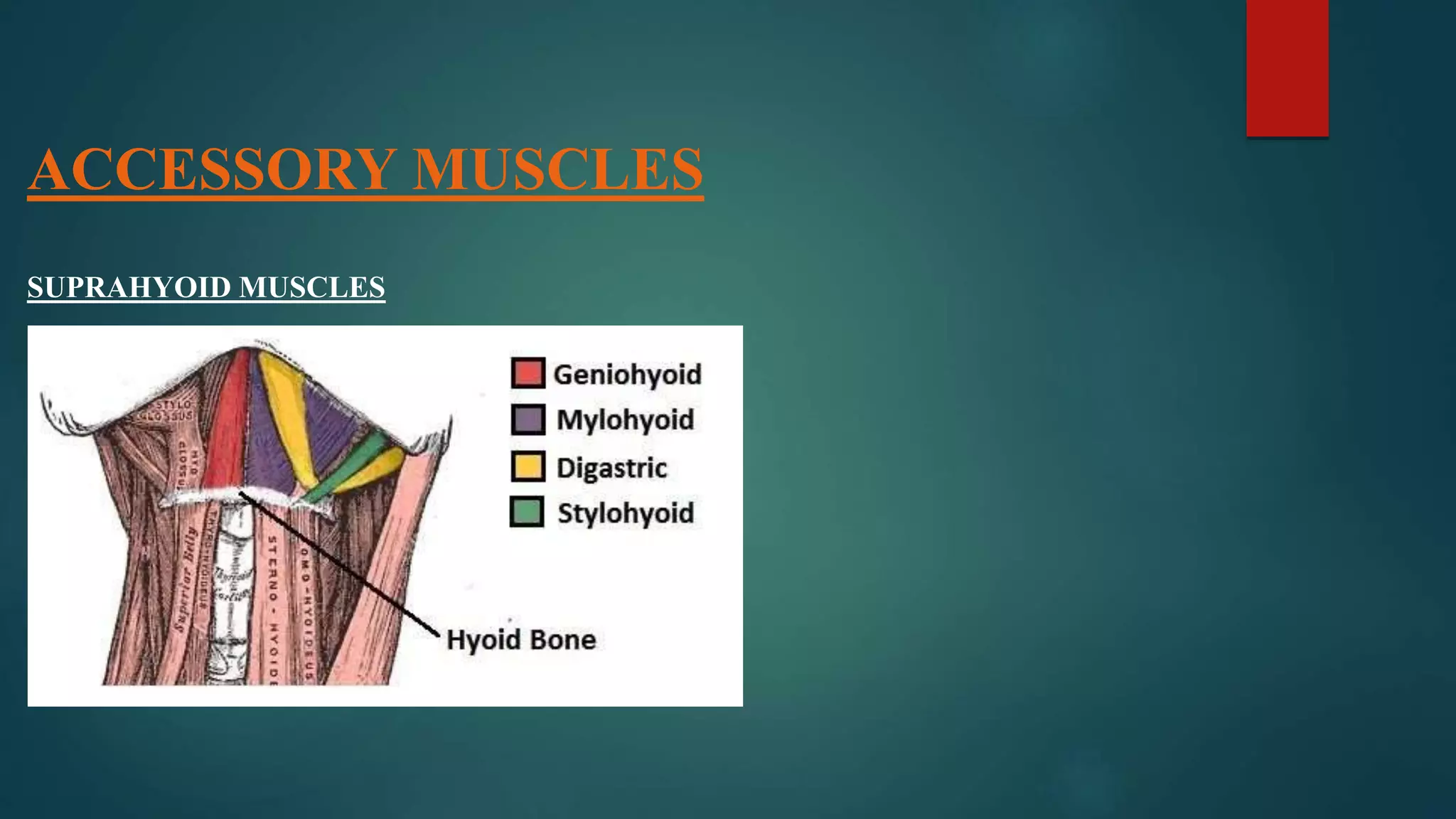

The document discusses the muscles of facial expression and mastication. It provides details on the origin, insertion, function and nerve supply of the main facial muscles including the orbicularis oculi, corrugator supercili, and zygomaticus major. It also discusses the muscles of mastication - masseter, temporalis, lateral pterygoid, and medial pterygoid - and their roles in elevating and moving the mandible for chewing. The document emphasizes the importance of understanding facial muscle anatomy for areas like prosthodontics and in treating patients with facial paralysis.











































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


