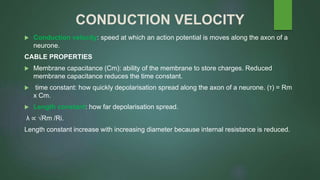
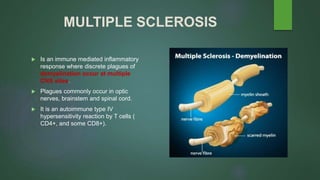
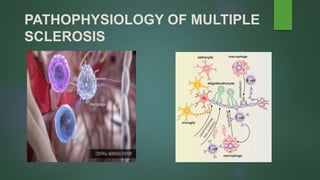
The document discusses multiple sclerosis (MS), a disease where patches of demyelination occur in the central nervous system. It describes optical neuritis and Schilder's disease, two conditions with similar symptoms to MS. It then covers nerve action potentials, myelination, and saltatory conduction. The pathophysiology of MS involves an autoimmune attack on myelin by T cells and antibodies. Symptoms depend on the location of lesions and include vision issues, coordination problems, and sensory or motor impairments. Diagnosis involves MRI, lumbar puncture, and evoked potentials. Treatment focuses on steroids, monoclonal antibodies, and interferon beta to slow demyelination.