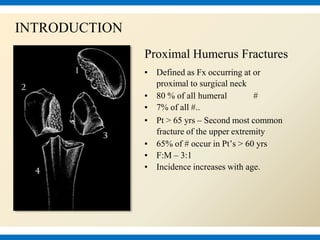
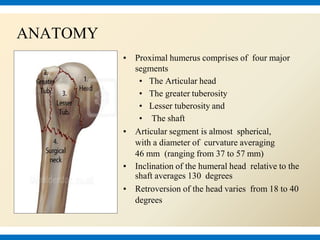
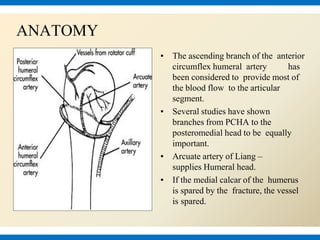
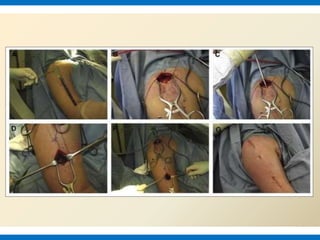
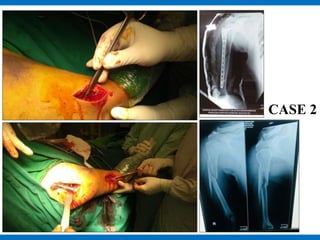
This document discusses the minimally invasive percutaneous osteosynthesis (MIPO) technique for treating proximal humerus fractures. It provides an overview of proximal humerus fracture anatomy, classification systems, treatment options, and the definition and procedure of MIPO. MIPO aims to minimize soft tissue disruption through small incisions and indirect reduction. The document presents two case examples where MIPO was used successfully to treat proximal humerus fractures. It concludes that MIPO is a safe and effective option with benefits like fewer complications and better functional recovery compared to open reduction and internal fixation, though reduction can sometimes be difficult.

























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)











