Downloaded 32 times
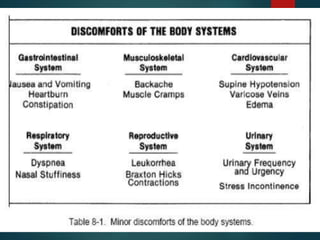




Nausea and vomiting, heartburn, constipation, edema, and urinary frequency are some of the most common minor disorders experienced during pregnancy. Nursing interventions for these conditions include dietary changes like eating small, frequent meals; hydration; exercise; rest; and reassurance that the symptoms are normal and temporary. Proper posture and stress relief techniques can also help alleviate discomfort. Notifying the medical provider is recommended if problems arise like pain, bleeding, or other abnormal symptoms. Overall, minor pregnancy complaints are usually nothing to worry about with simple lifestyle adjustments.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)












