Download to read offline

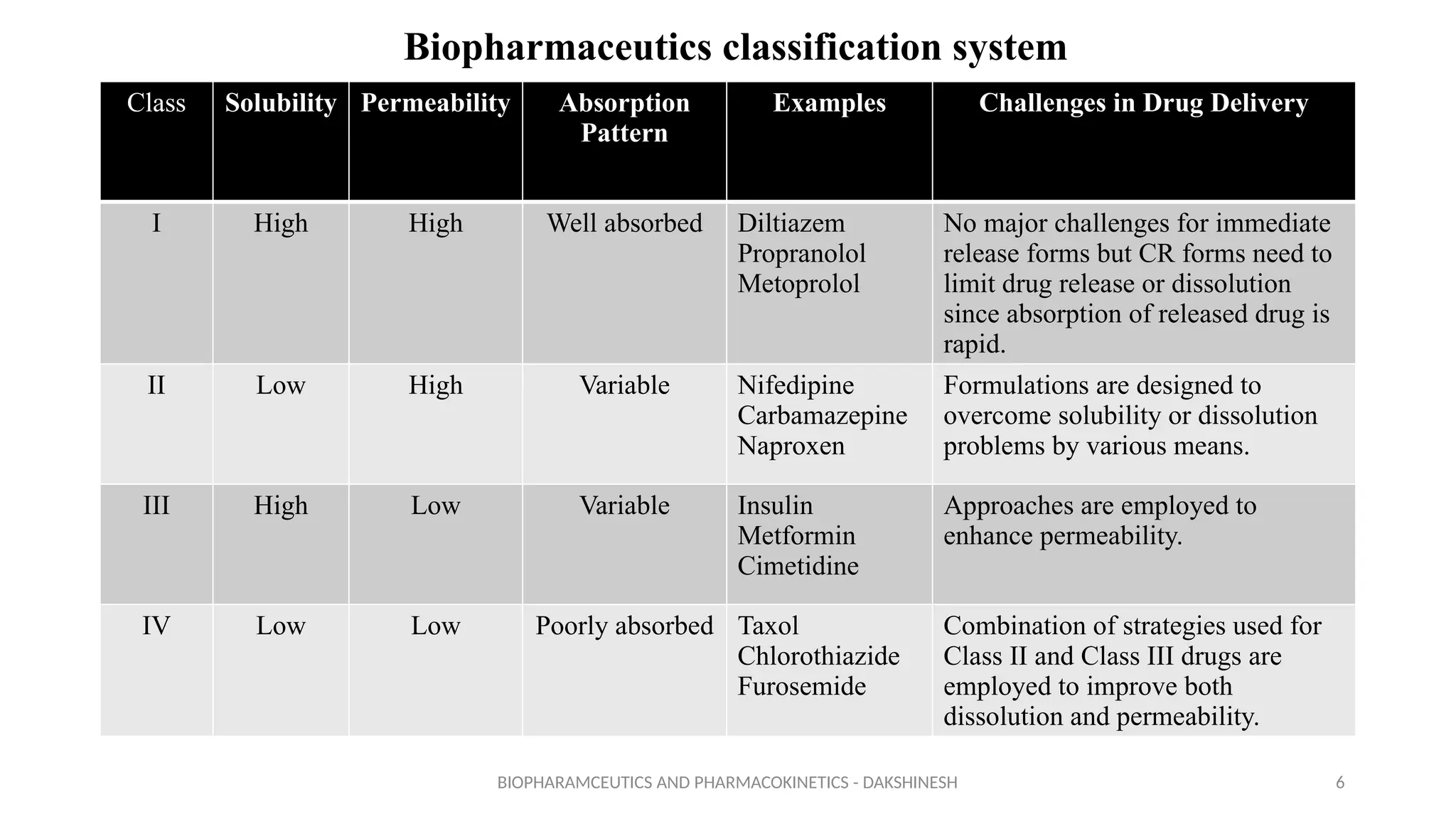















































This document discusses biopharmaceutics and pharmacokinetics, focusing on enhancing the dissolution rates and bioavailability of poorly soluble drugs. It outlines reasons for poor bioavailability, the Biopharmaceutics Classification System (BCS), and various approaches to overcome these issues, including pharmaceutical, pharmacokinetic, and biological strategies. Specific techniques for enhancing drug solubility and permeability are detailed, such as micronization, nanonization, and the use of surfactants.