



























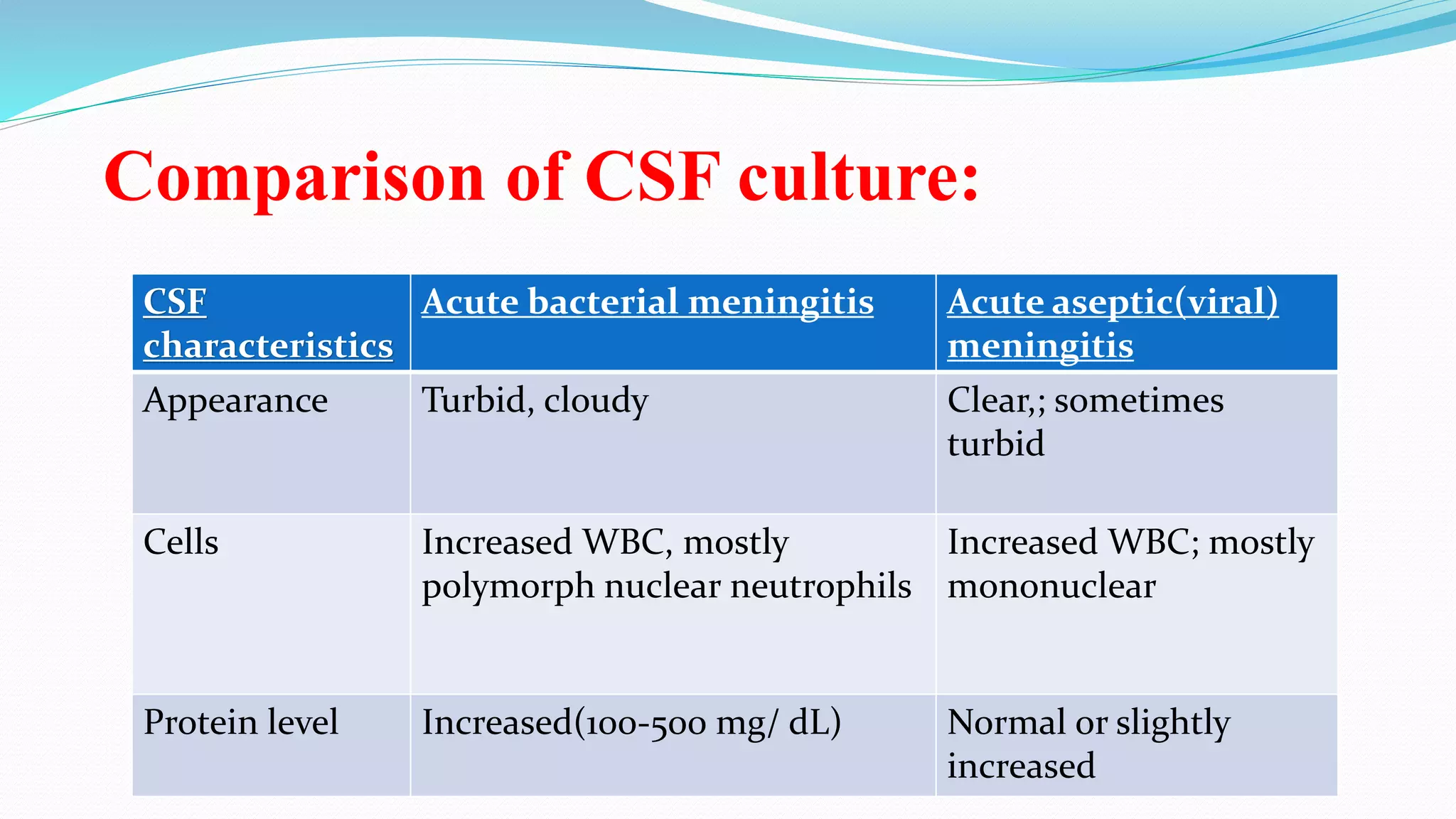
















This document discusses meningitis, including its classification, causative organisms, incidence, risk factors, pathophysiology, clinical features, diagnosis, treatment, prevention, and nursing management. It defines meningitis as an inflammation of the membranes surrounding the brain and spinal cord, most commonly caused by bacteria or viruses. The main types are acute bacterial meningitis, which requires emergency treatment, and chronic meningitis, present for over a month. Common causative organisms are pneumococcal, meningococcal, and H. influenza bacteria. Clinical features include headache, fever, neck stiffness, and altered mental status. Diagnosis involves examination of cerebrospinal fluid. Treatment involves antibiotics and supportive care. Nursing focuses on



































































