Downloaded 26 times
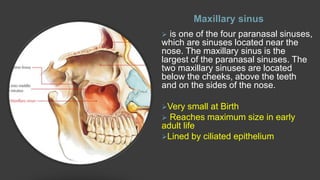
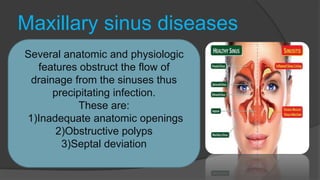
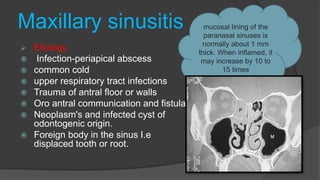
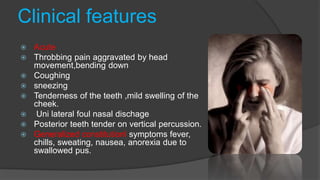

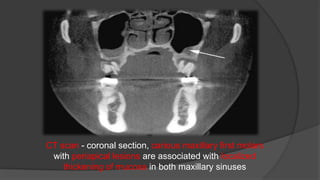
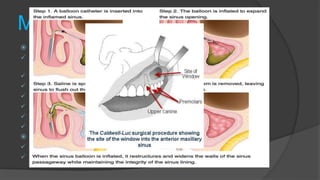

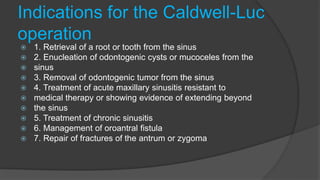
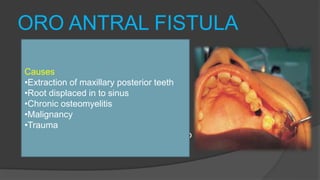
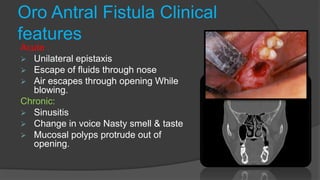

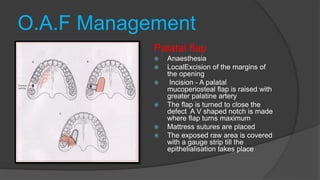
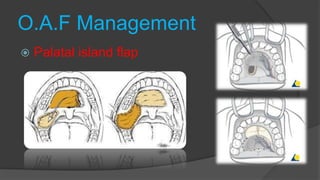
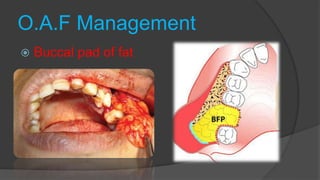

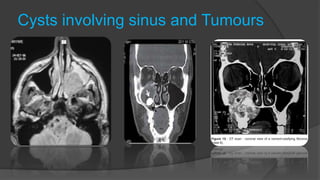


The maxillary sinus is the largest of the paranasal sinuses. It is located below the cheeks and above the teeth. Maxillary sinusitis is usually caused by infection, trauma, or dental issues like cysts or displaced roots. Symptoms include pain, nasal discharge, and tenderness of teeth. Diagnosis involves examination, transillumination, and radiography. Treatment may include antibiotics, surgery like Caldwell-Luc to drain pus, or repair of oroantral fistulas caused by tooth extractions. Complications can arise if fistulas are not properly closed.





























![maxillarysinus-170705134531 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/maxillarysinus-170705134531autosaved-240606120847-09cc00a0-thumbnail.jpg?width=640&height=640&fit=bounds)







![MAXILLARY SINUS AND ITS SURGICAL ANATOMY (2) (1) [Autosaved].ppt](https://cdn.slidesharecdn.com/ss_thumbnails/maxillarysinusanditssurgicalanatomy21autosaved-240927151609-5597be7b-thumbnail.jpg?width=640&height=640&fit=bounds)















![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













