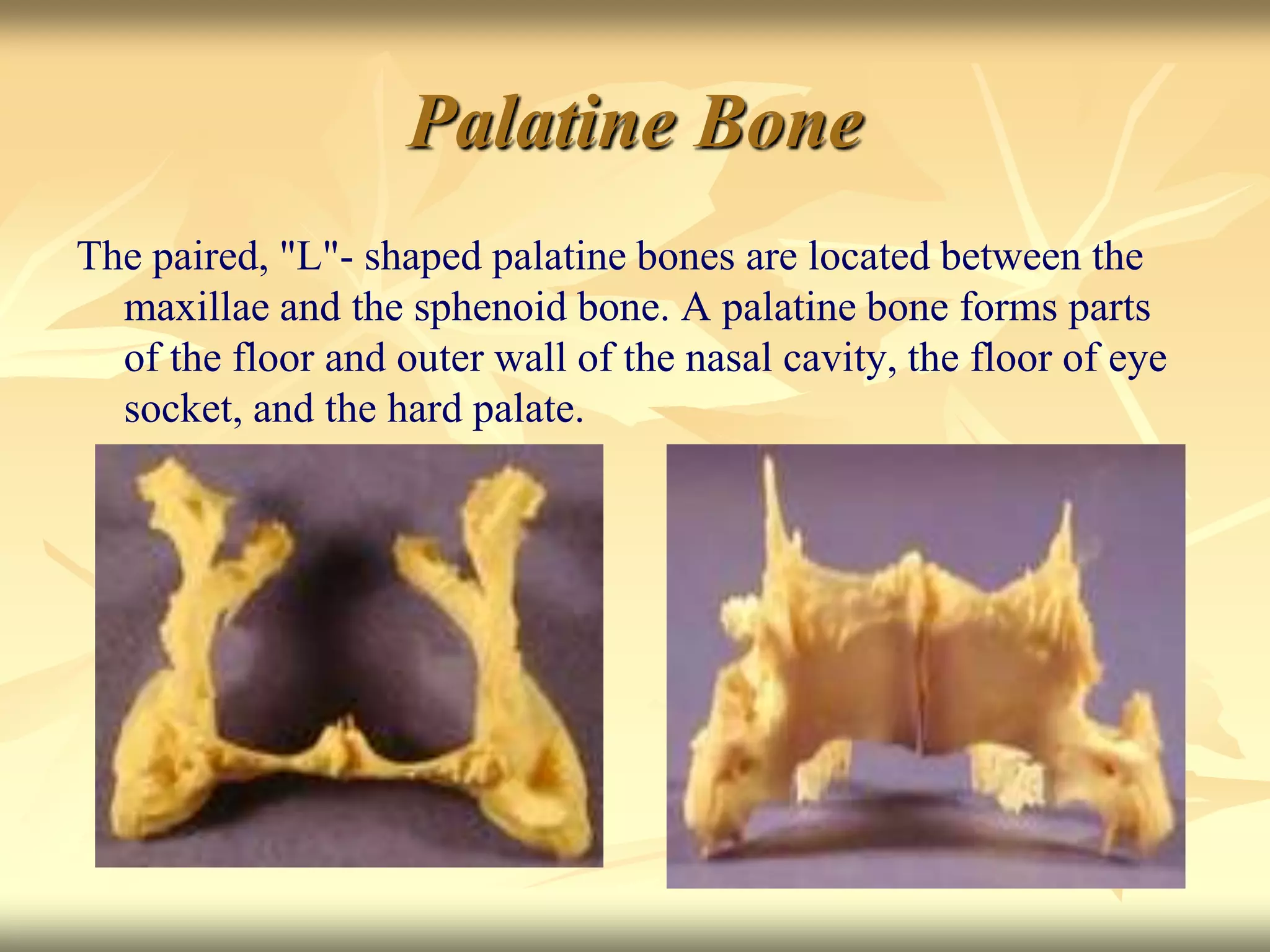
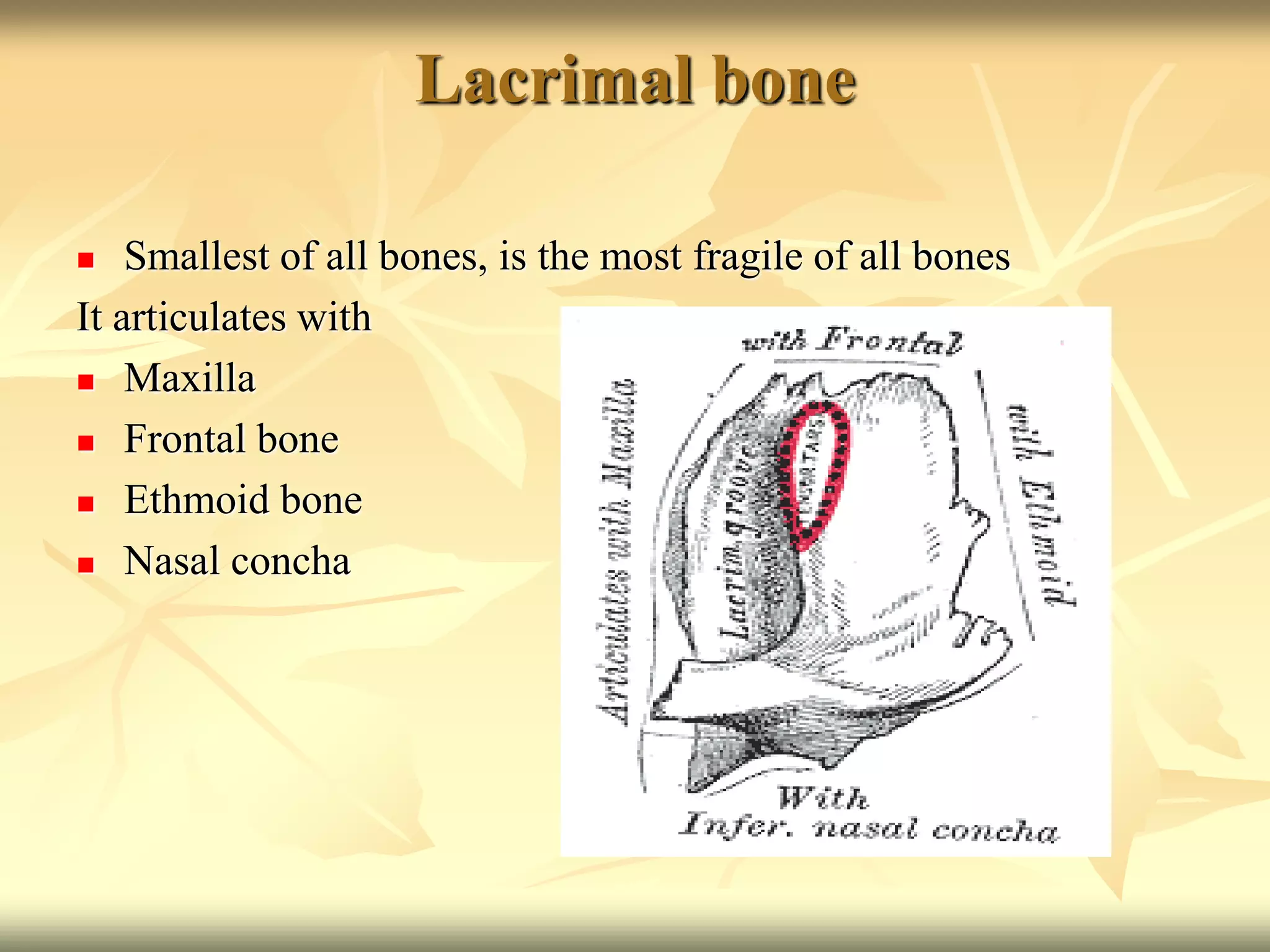
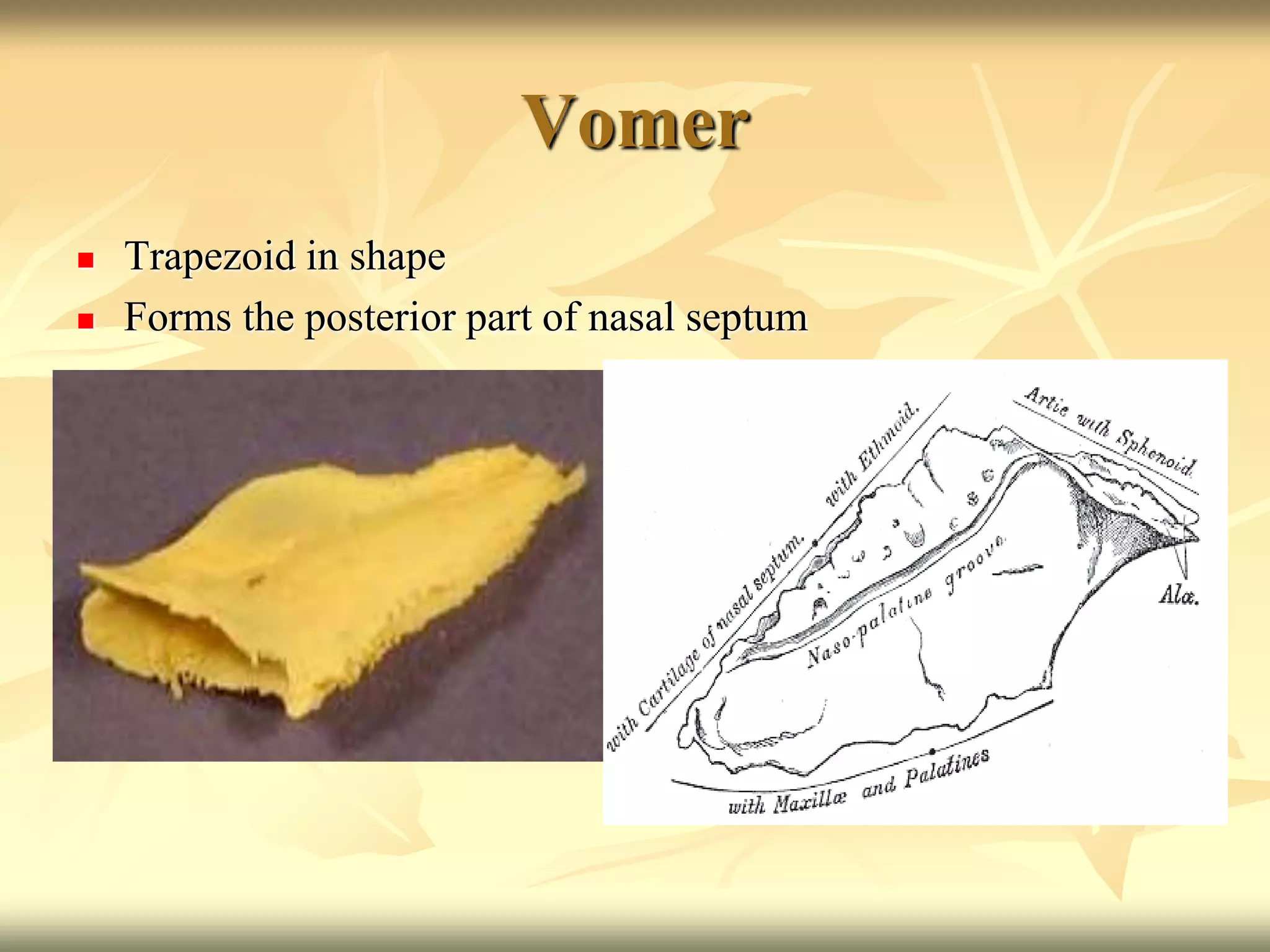
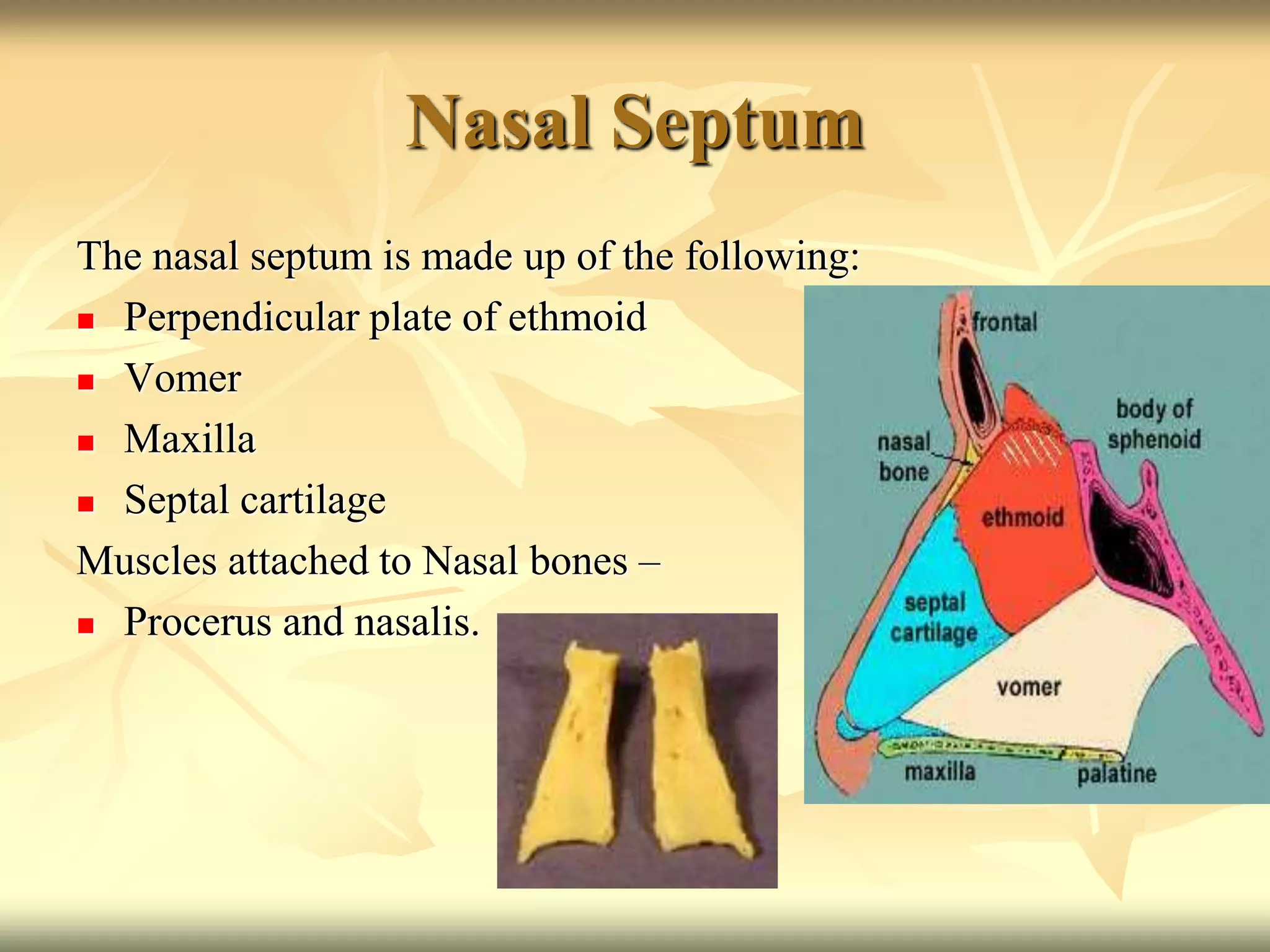
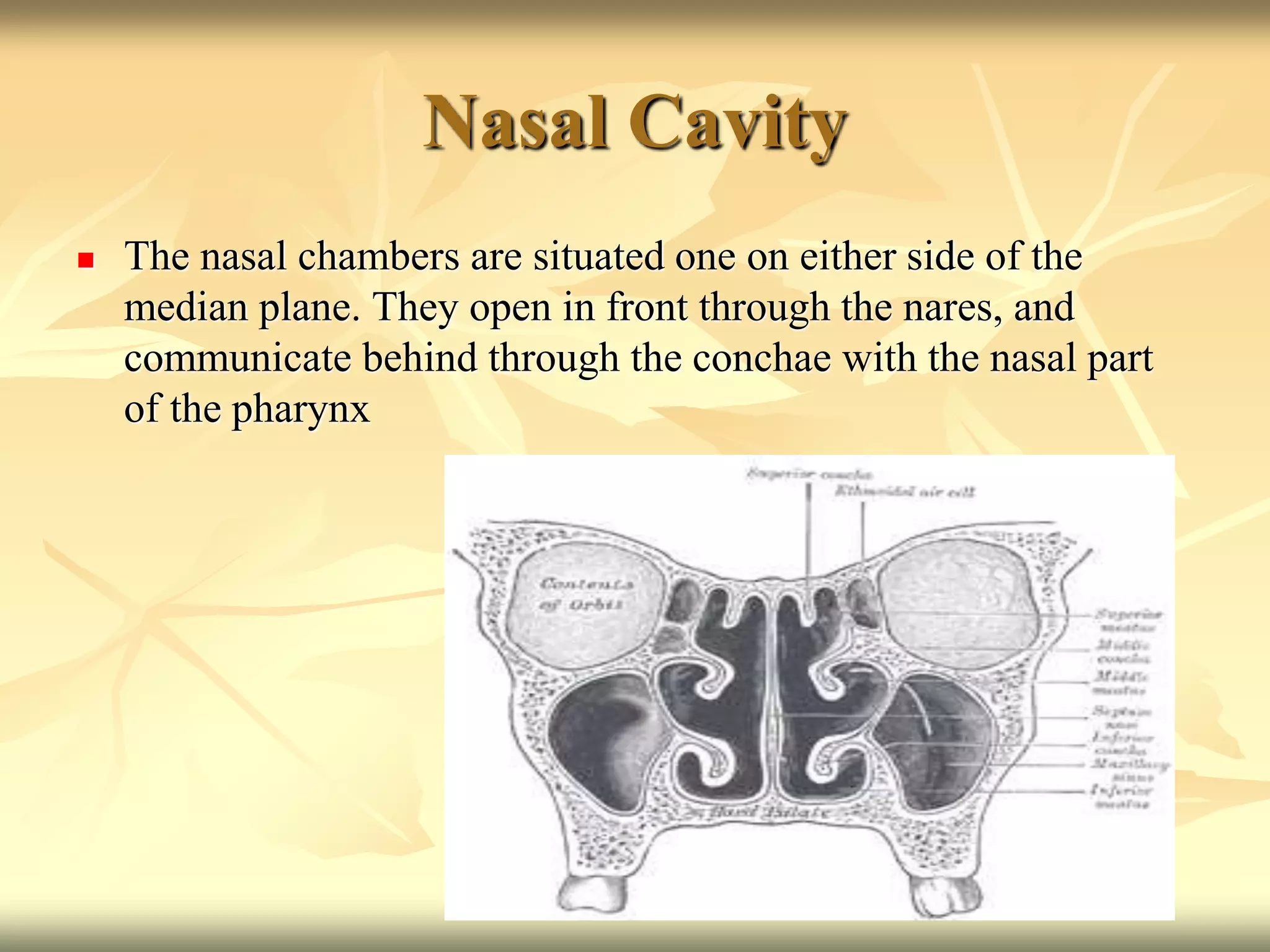
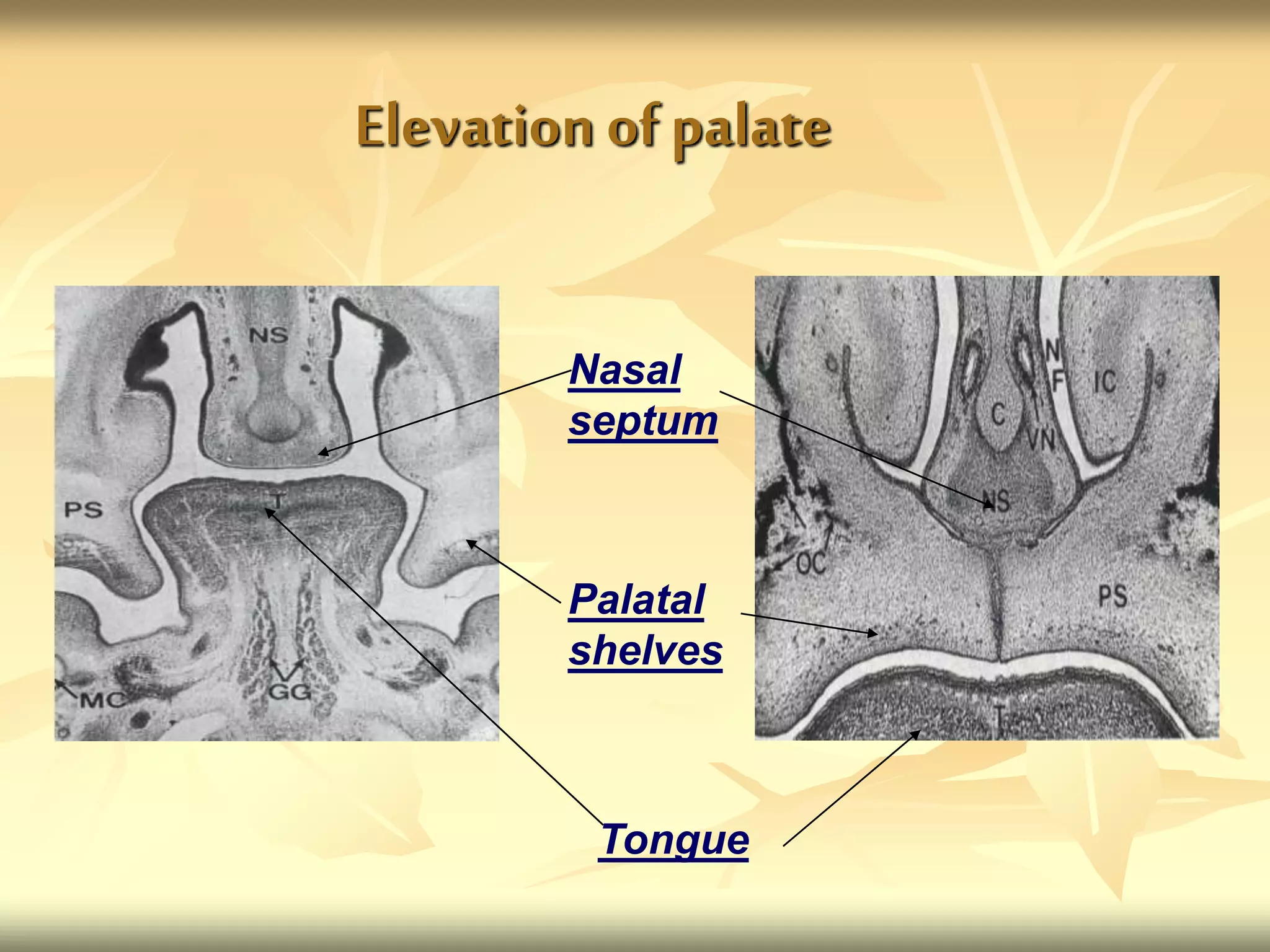
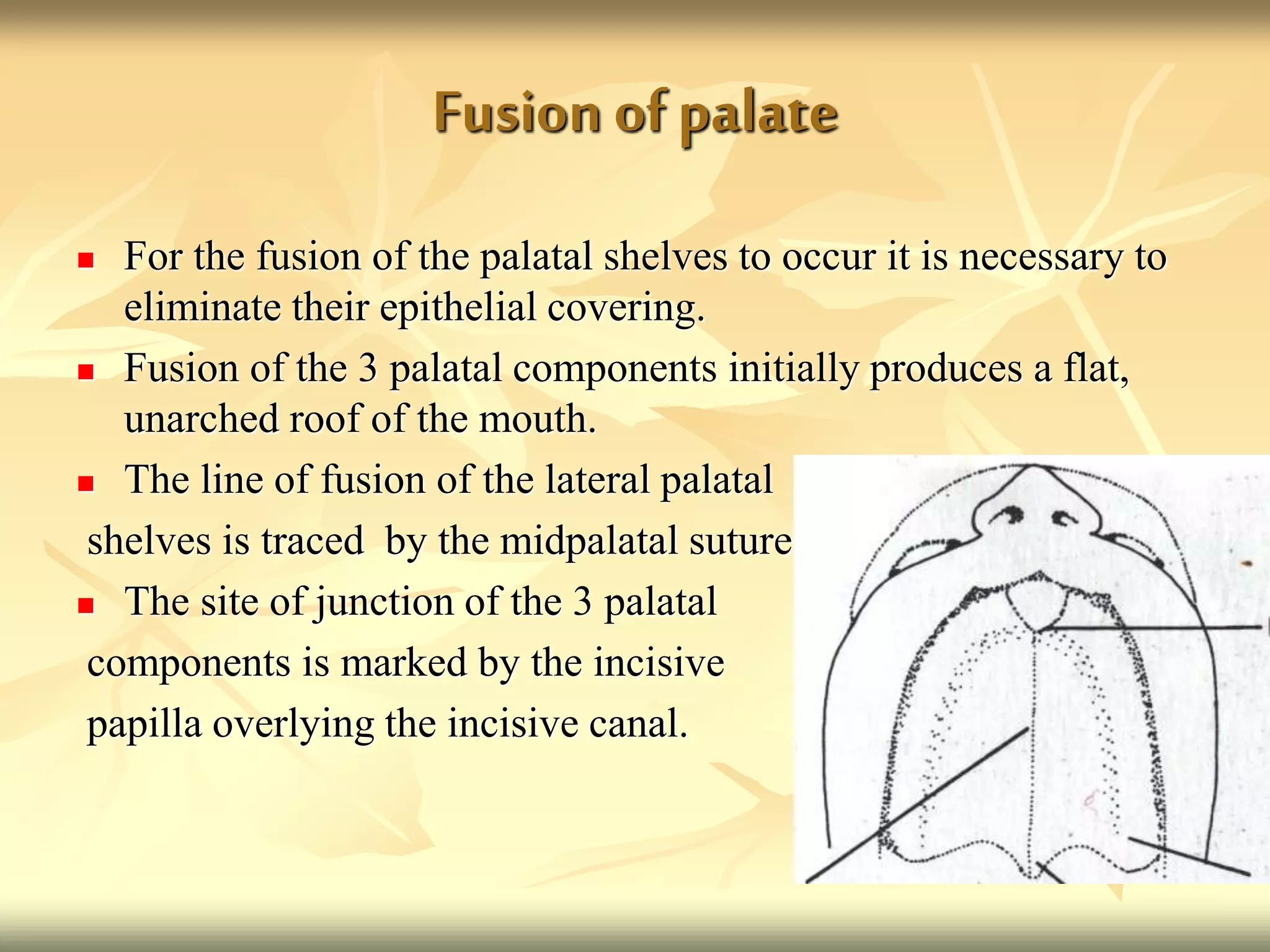
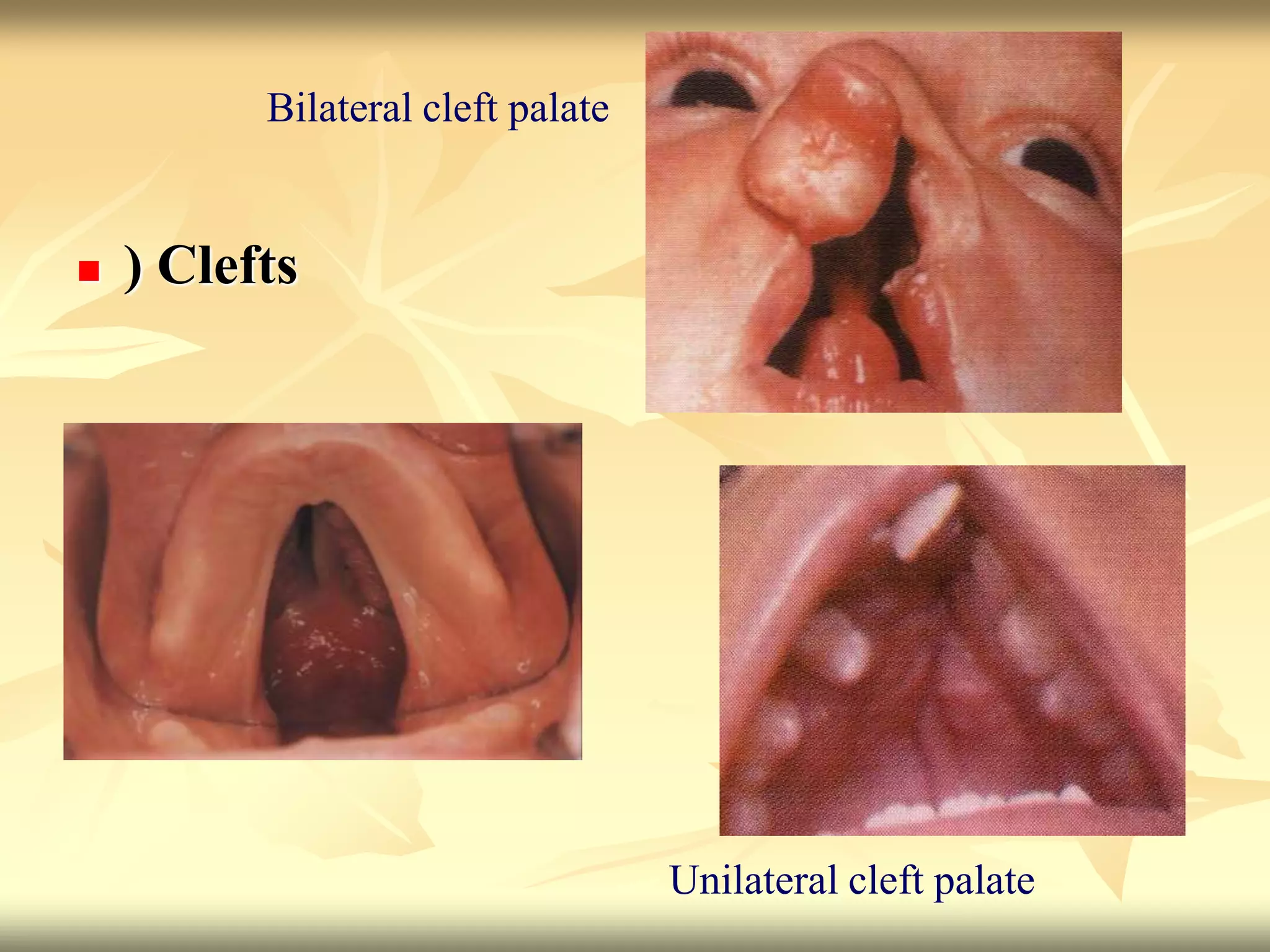
The document summarizes the growth and development of the nasomaxillary complex. It discusses the anatomy of bones that make up the nasal cavity and palate. It describes the prenatal development of these structures, including the formation of the primary and secondary palate from palatal shelves and their elevation and fusion between 5-12 weeks. Postnatal growth of the maxilla, palate and sinuses is also summarized.

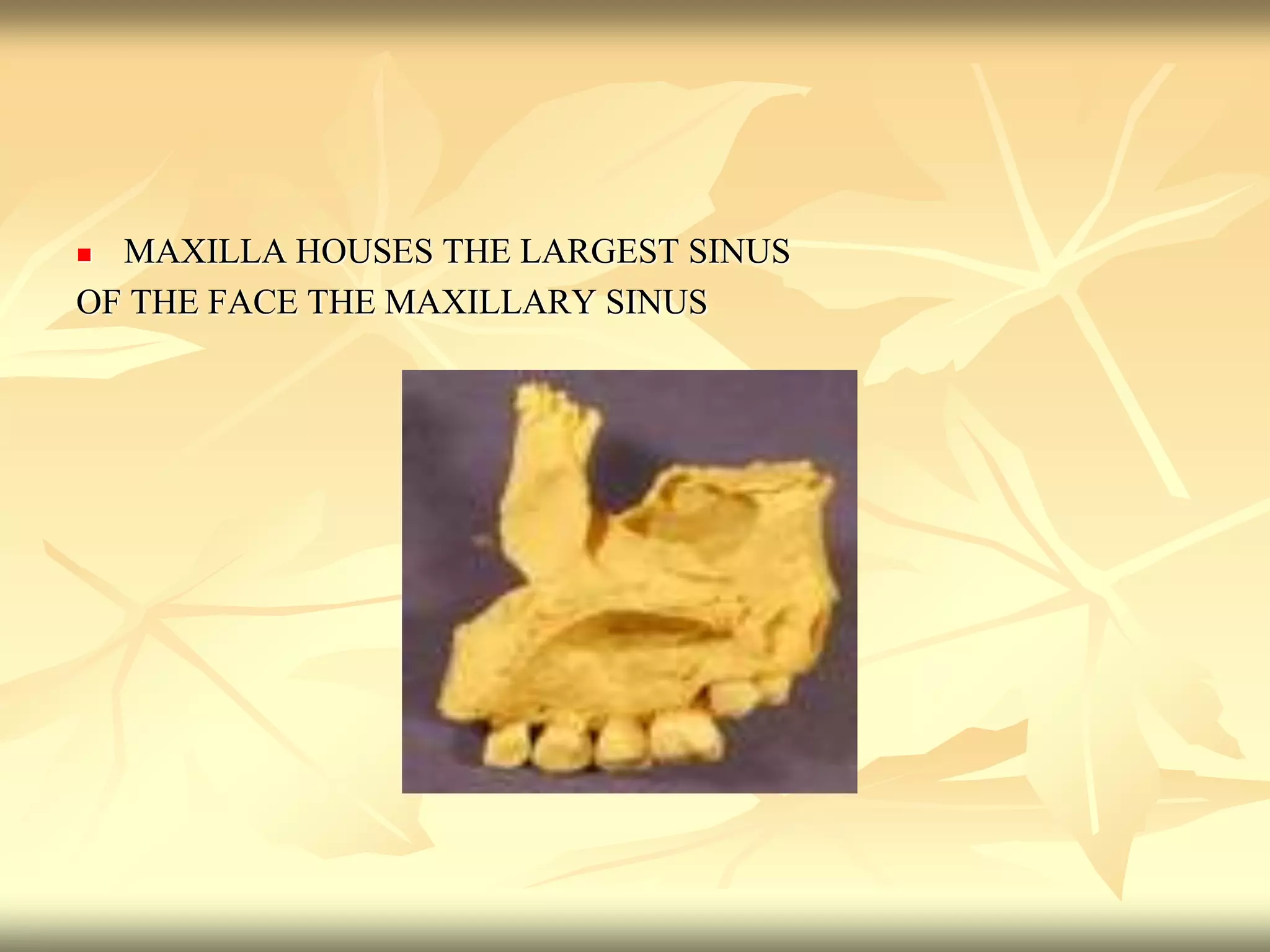
![Maxillary sinus
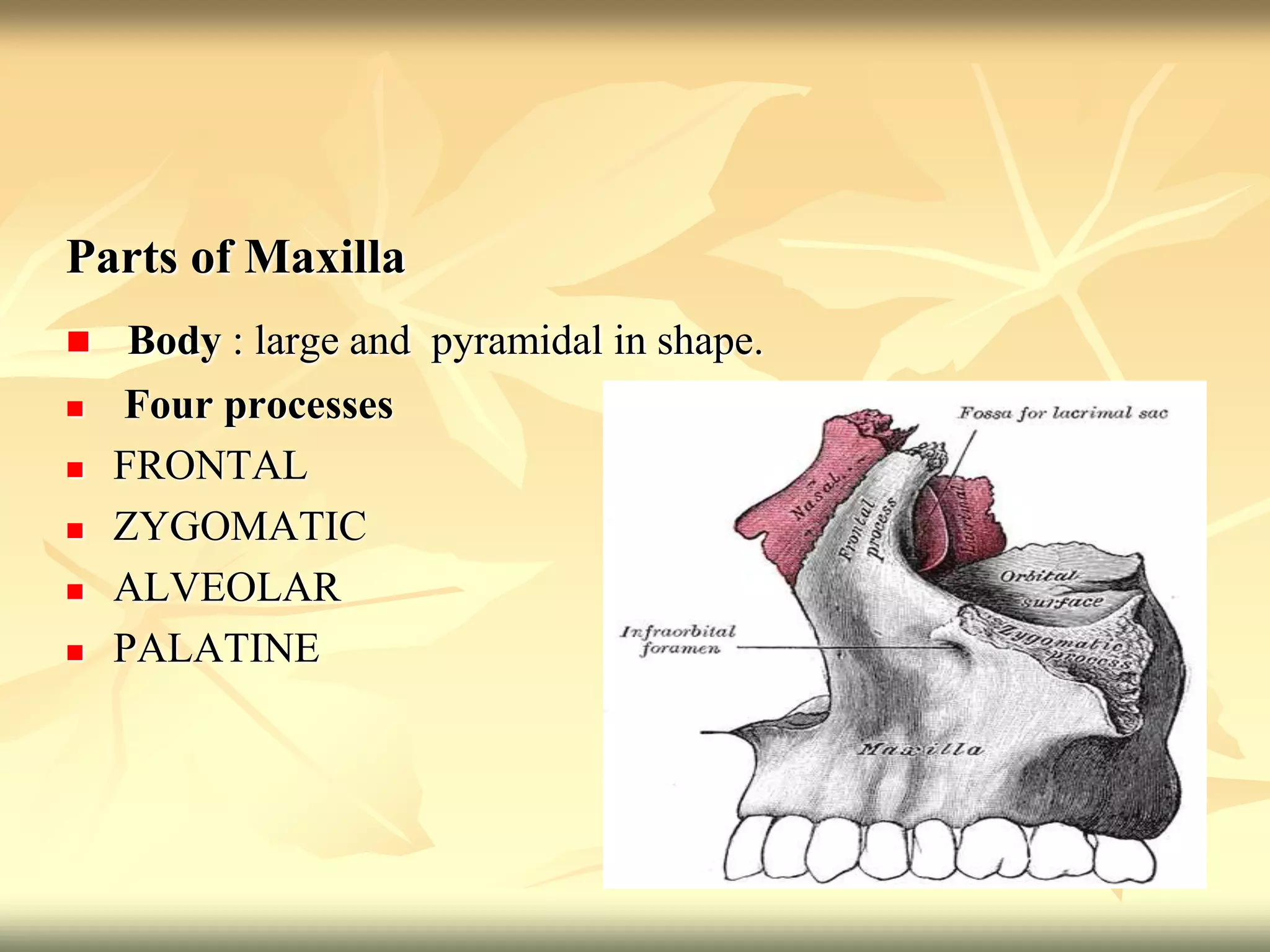
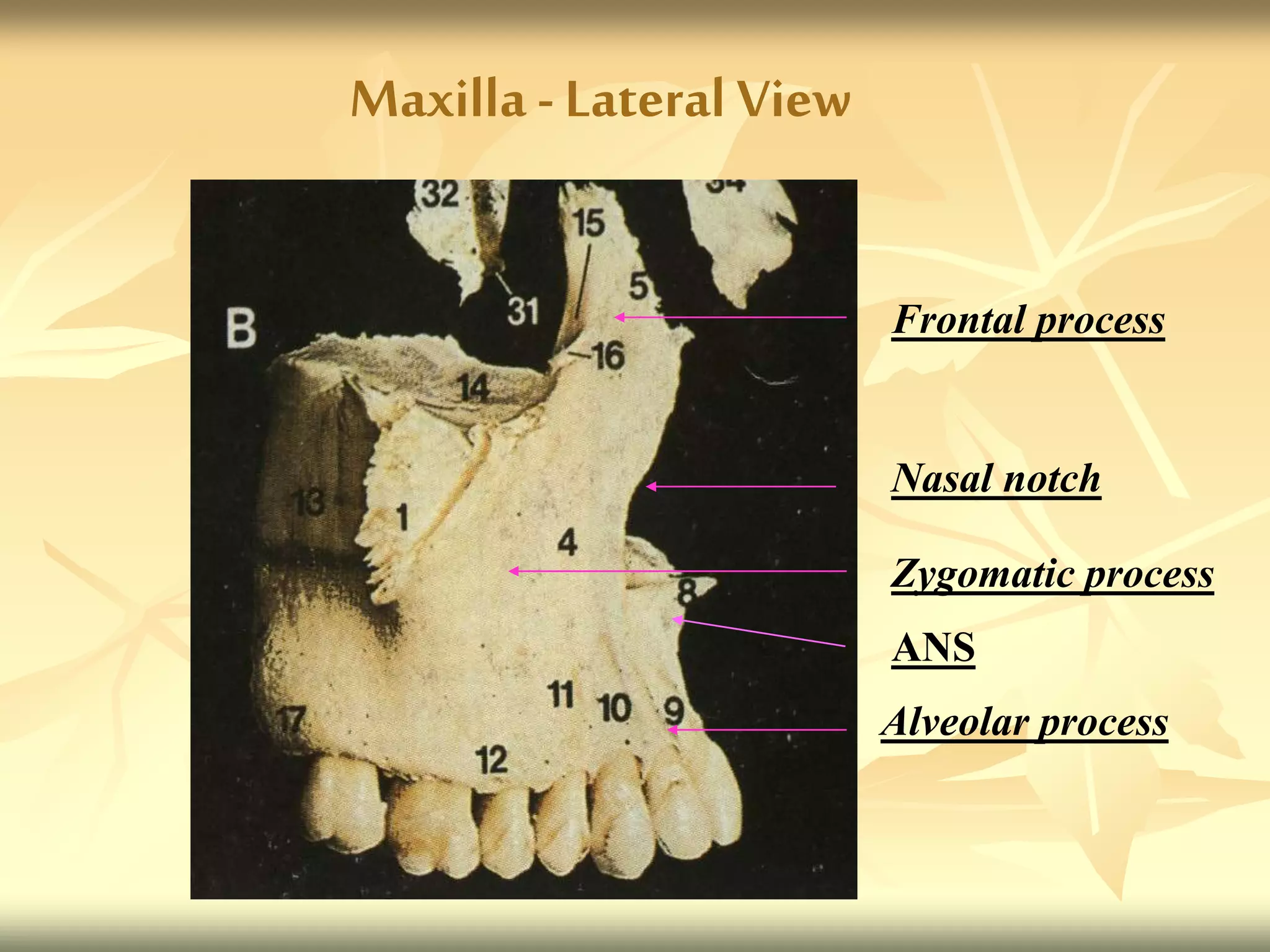
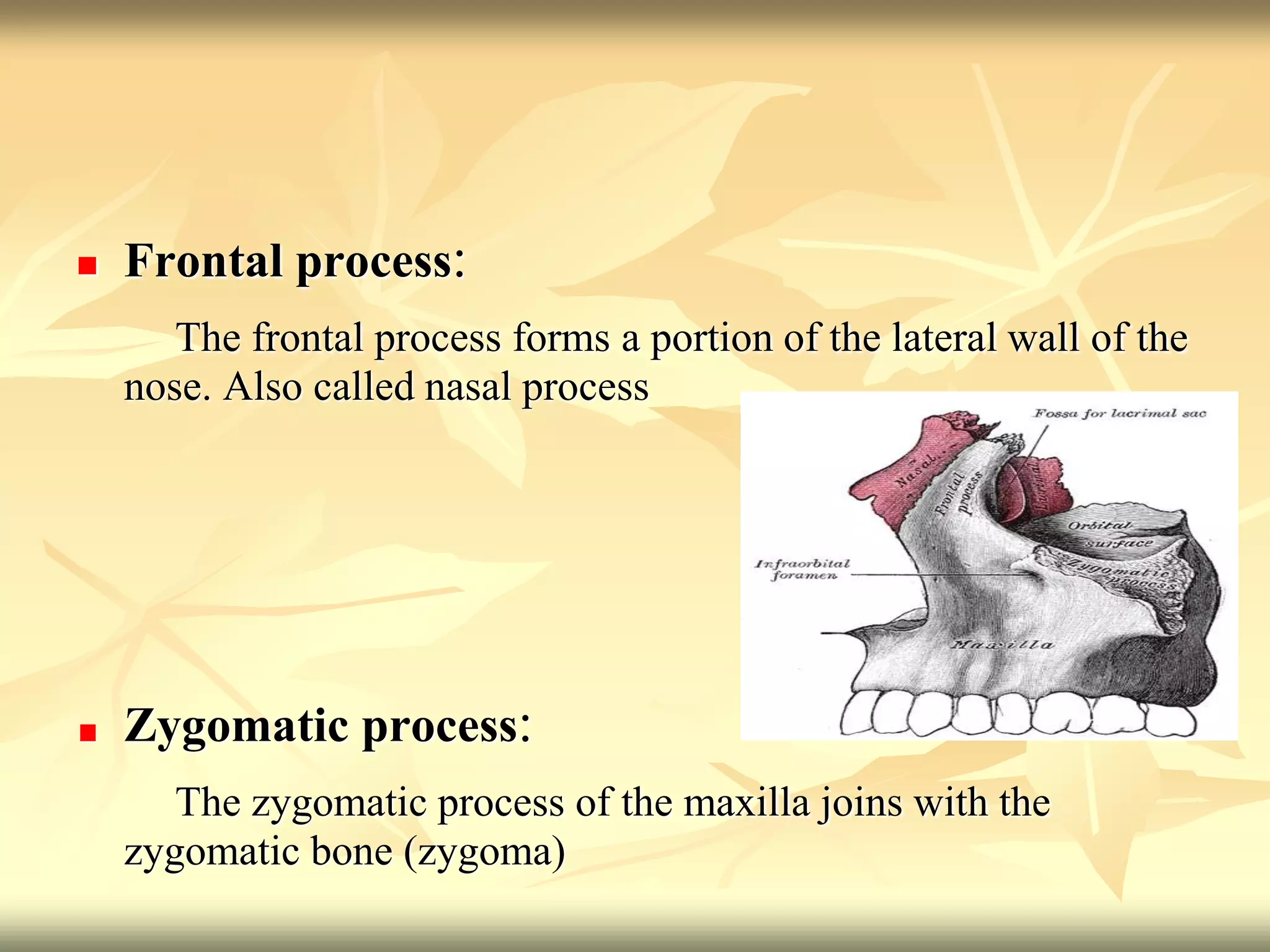
Frontal process
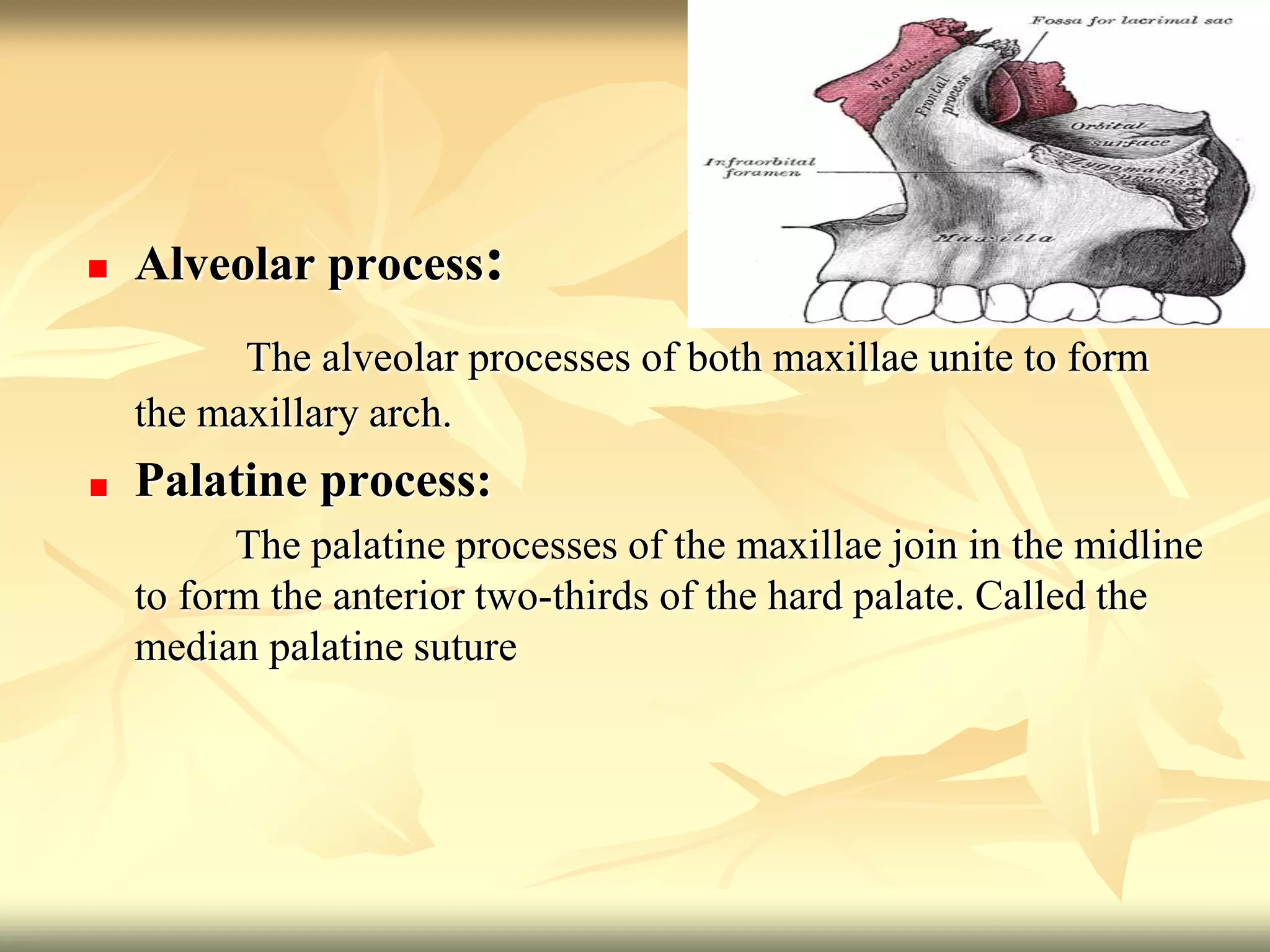
Alveolar process
Maxilla –Medial View
Maxillary process [palatine]
Horizontal plate of palatine
Palatine process[maxilla]](https://image.slidesharecdn.com/growthanddevelopmentofnasomaxillarycomplexppt-220829052134-125effd1/75/Growth-and-Development-of-Nasomaxillary-complex-PPT-ppt-7-2048.jpg)



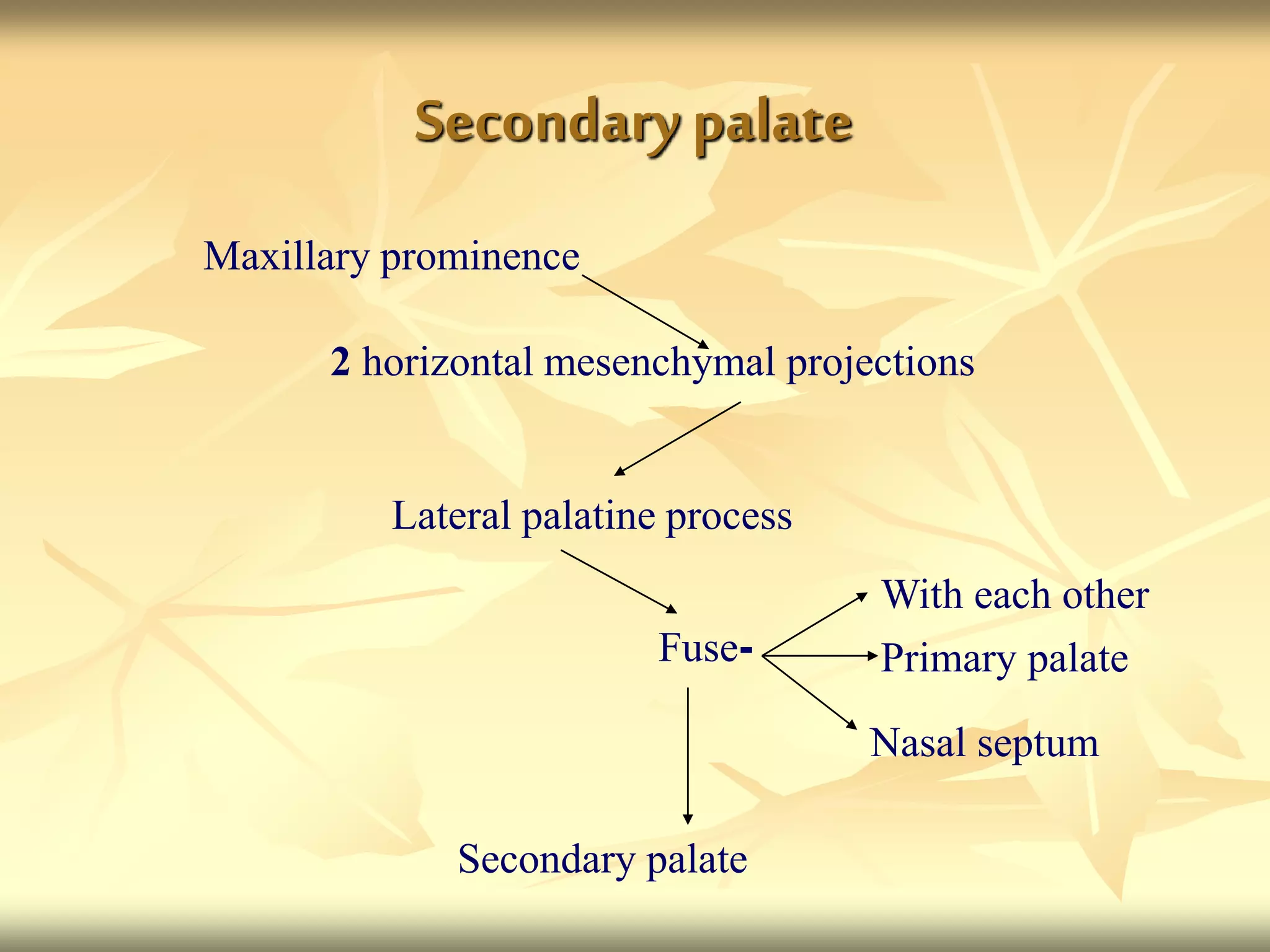

![Formation of palate[summary]
Primordium
of
Formed
by
Derived
from
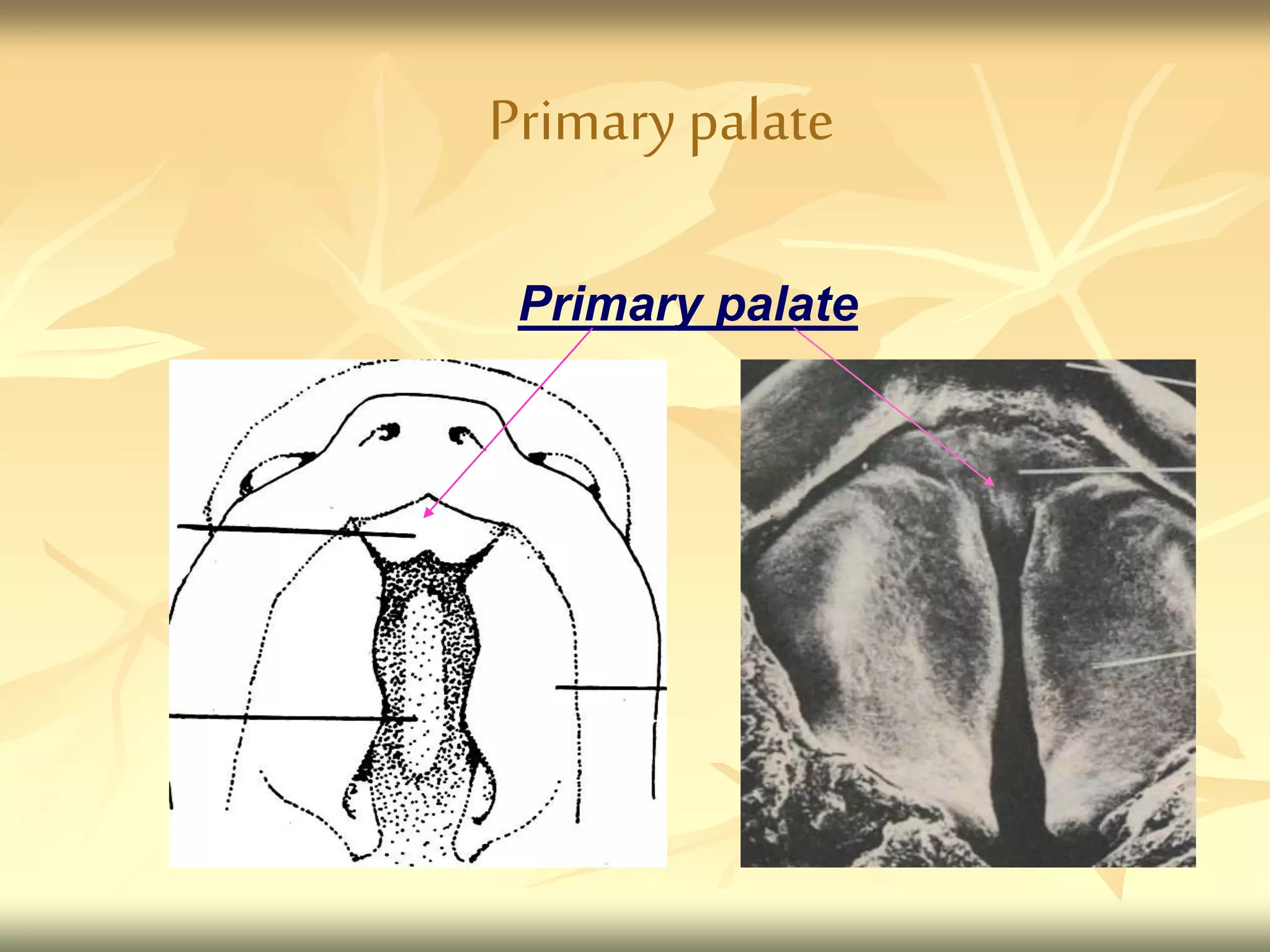
Primary
palate
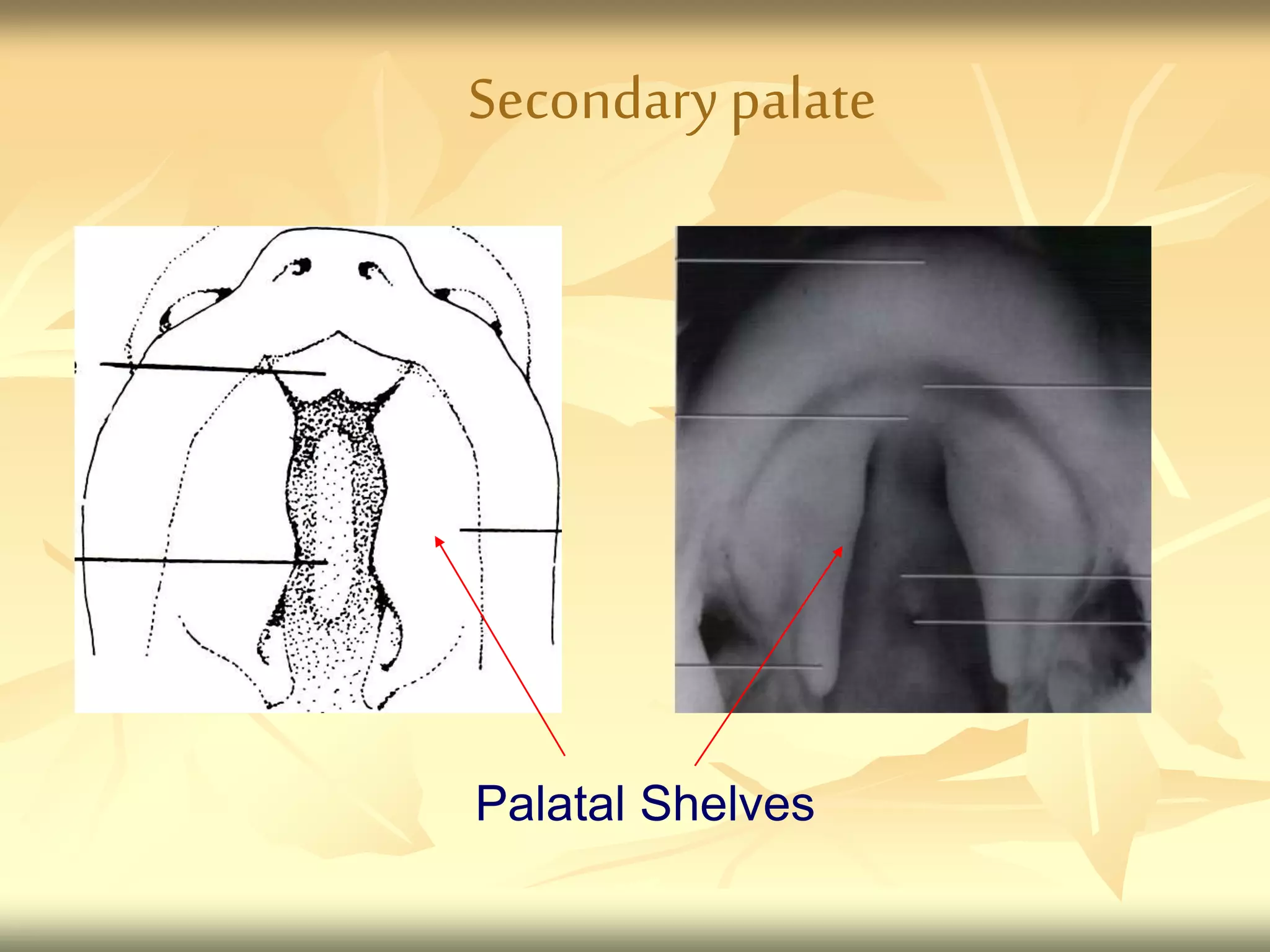
Secondary
palate
Pre
maxilla
Hard and
soft
palate
Median
palatine
process
Lateral
palatine
process
Maxillary
process
Frontonasal
process](https://image.slidesharecdn.com/growthanddevelopmentofnasomaxillarycomplexppt-220829052134-125effd1/75/Growth-and-Development-of-Nasomaxillary-complex-PPT-ppt-50-2048.jpg)

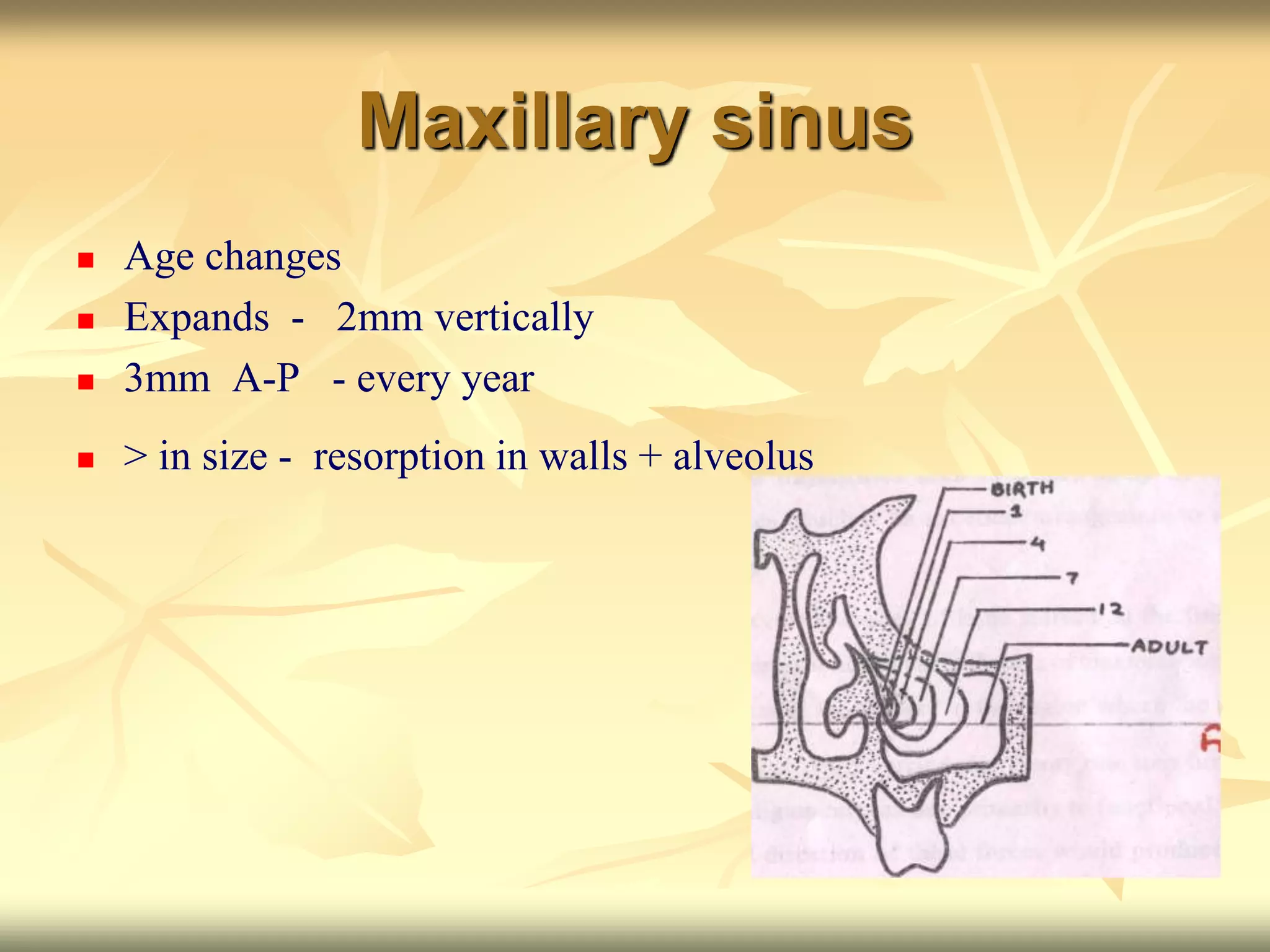
![ POST NATAL
All internal surfaces -resorption
[expect medial]
Rapid continuous downward growth
close proximity to buccal maxillary
teeth](https://image.slidesharecdn.com/growthanddevelopmentofnasomaxillarycomplexppt-220829052134-125effd1/75/Growth-and-Development-of-Nasomaxillary-complex-PPT-ppt-87-2048.jpg)