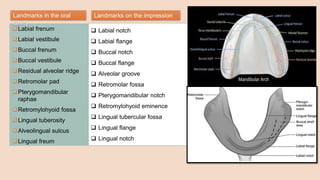
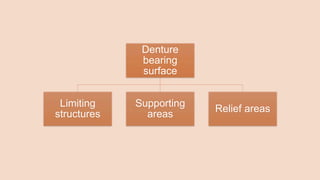
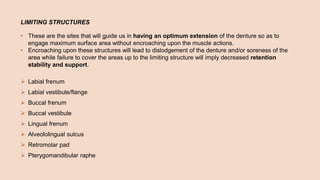
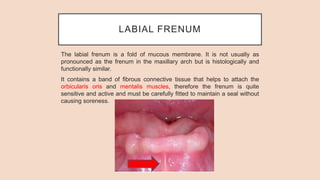
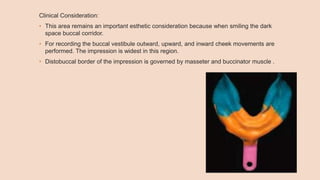
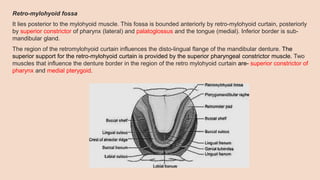
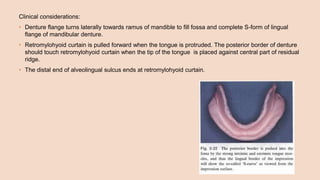
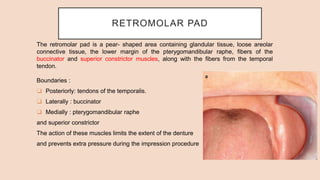
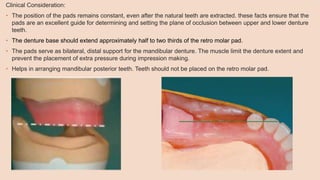
The document outlines key anatomical landmarks of the edentulous mandibular arch, which are crucial for the successful fabrication and fit of complete dentures. It discusses various structures such as the labial frenum, buccal frenum, and residual alveolar ridge that influence denture design, emphasizing their significance in creating impressions and ensuring comfort during use. Additionally, it highlights clinical considerations regarding these landmarks to avoid complications like soreness or displacement of the dentures.
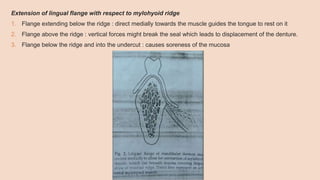



























![Anatomical landmarks of maxilla and mandible [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/anatomicallandmarksofmaxillaandmandibleautosaved-200820132830-thumbnail.jpg?width=640&height=640&fit=bounds)





























































