Downloaded 15 times

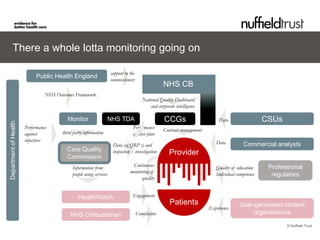

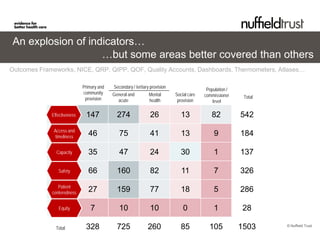
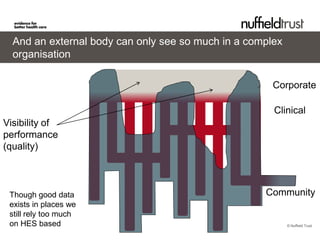
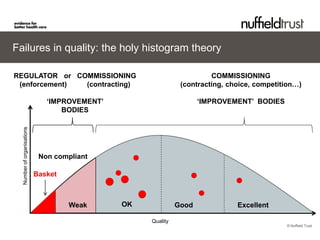
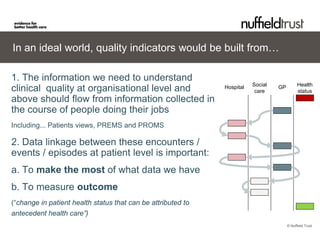

1) There are concerns that financial pressure from austerity measures may negatively impact healthcare quality, though more data is needed to establish clear relationships. 2) Multiple organizations currently monitor various quality indicators, but coverage is uneven across different settings and dimensions of quality. 3) Developing a comprehensive and standardized set of quality indicators that can be tracked over time across different care settings is an important goal, but collecting useful data, especially from patients and independent sectors, remains challenging.