
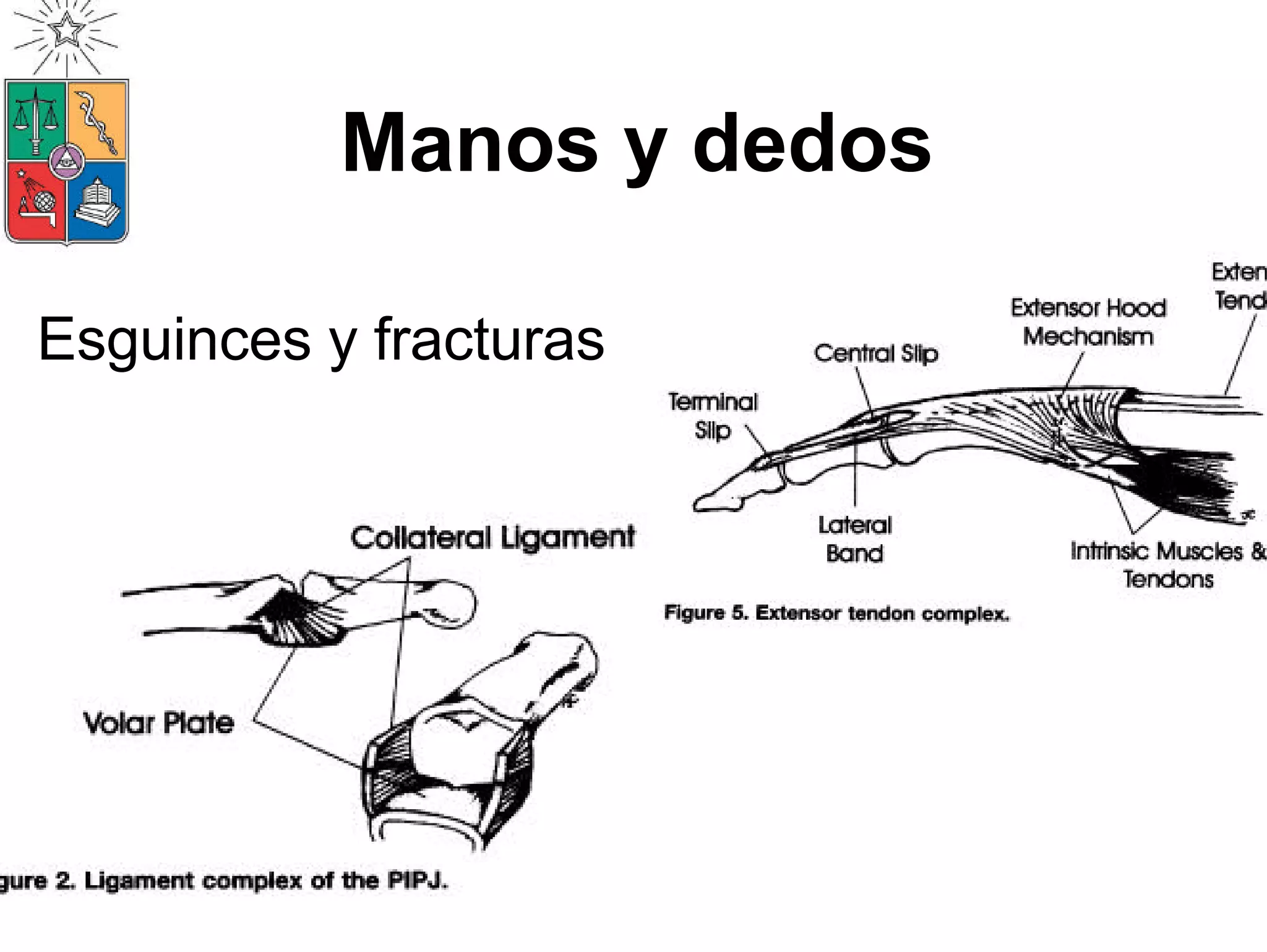
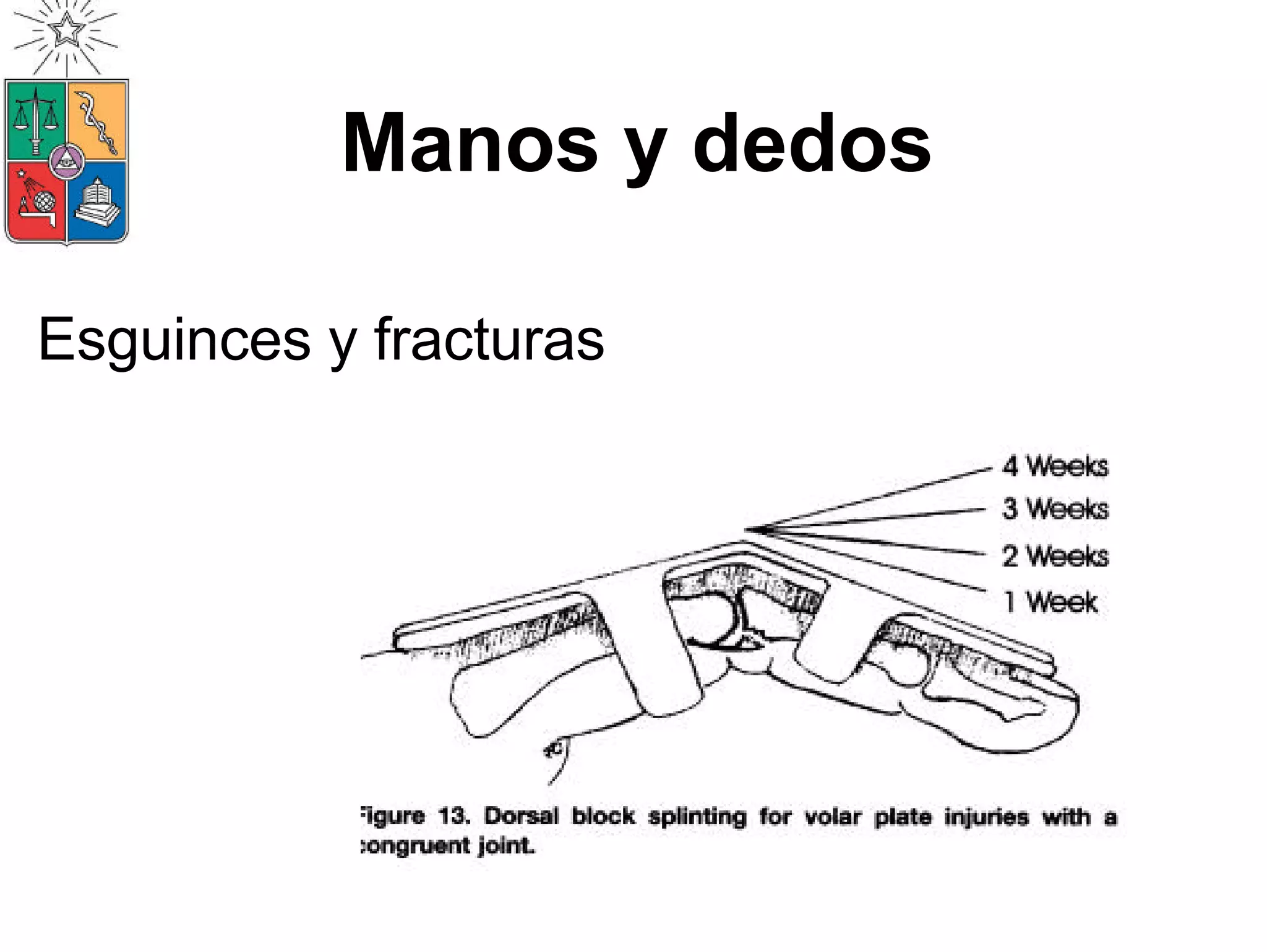

This document discusses elbow and hand injuries in athletes. It covers common elbow injuries like lateral epicondylitis, which occurs in over 50% of athletes performing overhead motions. It is characterized by pain at the lateral humeral epicondyle. Medial epicondylitis is also discussed, which affects golfers and tennis players. Rehabilitation is the first treatment, with surgery as an option if conservative treatment fails after 6-12 months. Injuries to the hand like sprains and fractures are also mentioned. The document concludes with an assignment separating students into groups to identify anatomical structures, risk factors, and management of specific sports injuries.























































































