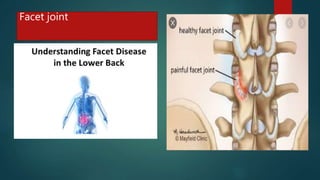
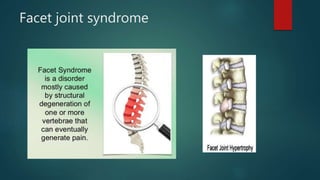
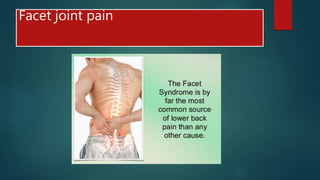
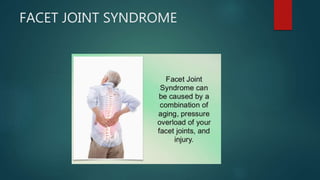
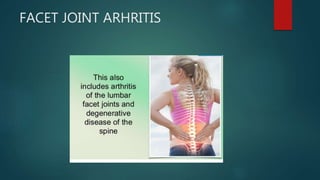
Facet joint syndrome is a cause of low back pain that occurs when the facet joints in the spine become irritated or inflamed. It is common, affecting up to 50% of patients with low back pain. It occurs due to repetitive strain on the joints from activities of daily living, poor posture, or spinal degeneration associated with aging. Symptoms include pain in the lower back area that is worsened with bending, twisting, or prolonged sitting or standing. Diagnosis involves imaging tests like x-rays, MRI, or CT scan. Treatment focuses on rest, medications, physical therapy including exercises and spinal manipulation, and procedures like injections to reduce inflammation.