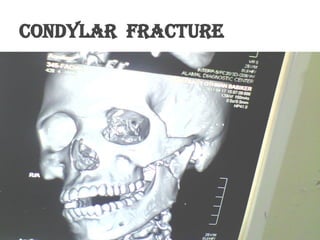
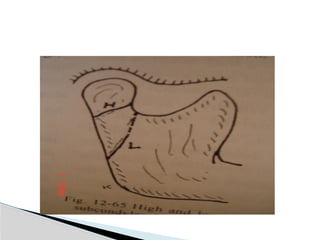
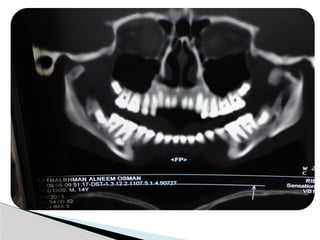
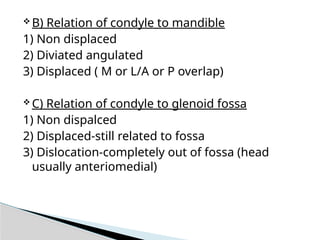
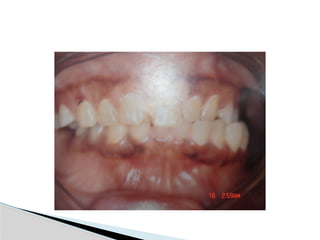
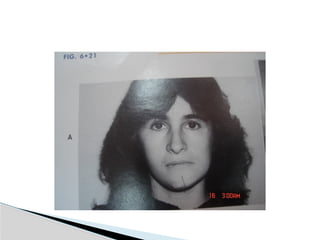
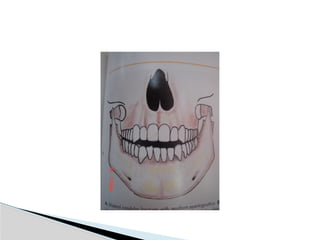
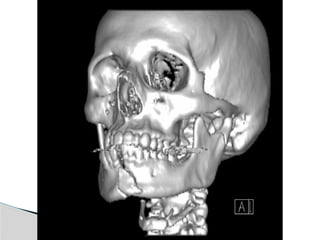
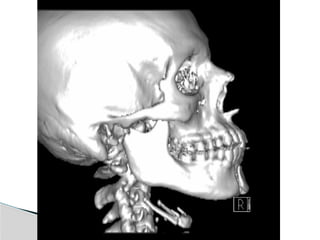
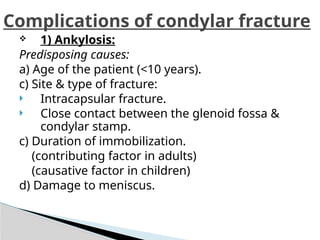
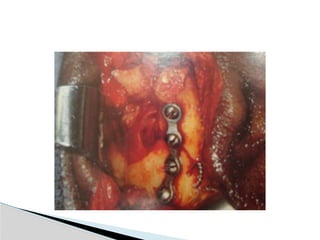
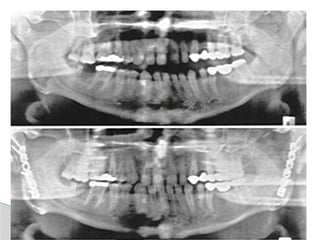
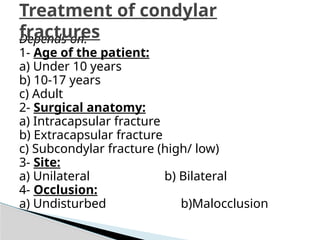
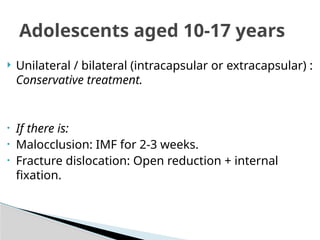
Condylar fractures are among the most common fractures of the mandible and typically result from indirect trauma, such as a blow to the chin, road traffic accidents, interpersonal violence, or falls. They may be classified based on anatomical location (condylar head, neck, or subcondylar region), degree of displacement, and presence of dislocation. Clinically, patients often present with preauricular pain, swelling, restricted mouth opening, deviation of the mandible on opening, malocclusion, and sometimes facial nerve dysfunction. Radiographic evaluation using panoramic radiographs and computed tomography is essential for accurate diagnosis and treatment planning. Management remains controversial and may be either conservative (closed reduction with functional therapy) or surgical (open reduction and internal fixation), depending on factors such as patient age, fracture type, degree of displacement, occlusal derangement, and associated injuries. Early mobilization and physiotherapy are crucial to restore mandibular function and prevent long-term complications such as ankylosis, malocclusion, and temporomandibular joint dysfunction.