Downloaded 232 times


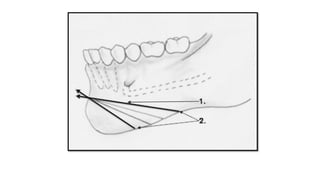
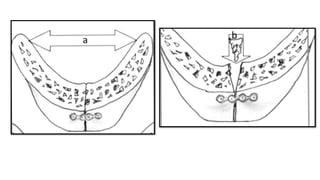
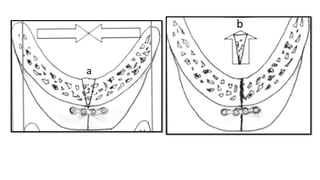
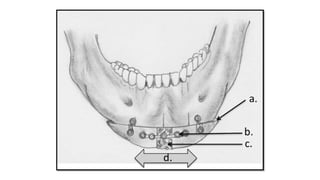
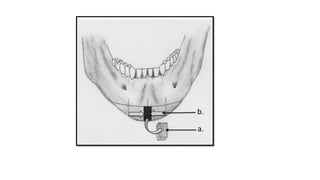
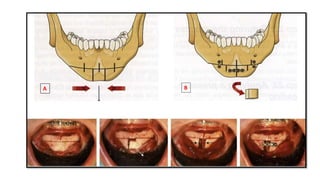
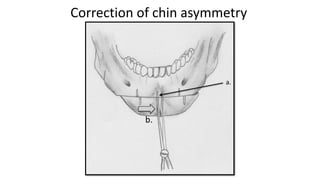
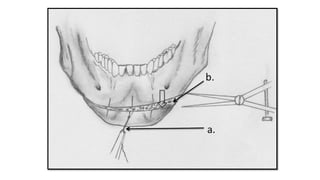
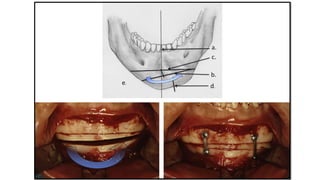
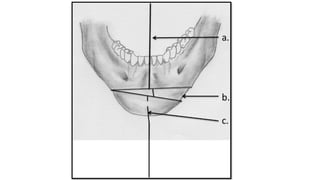

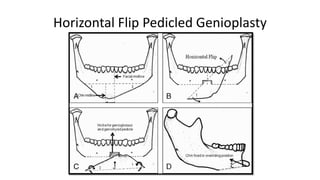


Genioplasty is a surgical procedure to alter the shape and projection of the chin bone. It can be done to augment a recessed chin or reduce a prominent chin, improving facial aesthetics and proportions. The surgery involves making precise bone cuts below the mental nerves and sliding the bony segment to reposition the chin. Careful preoperative evaluation and planning is required to determine the optimal surgical approach and amount of correction needed. Potential risks include injury to the mental nerves or poor healing of the bone cuts.











































































