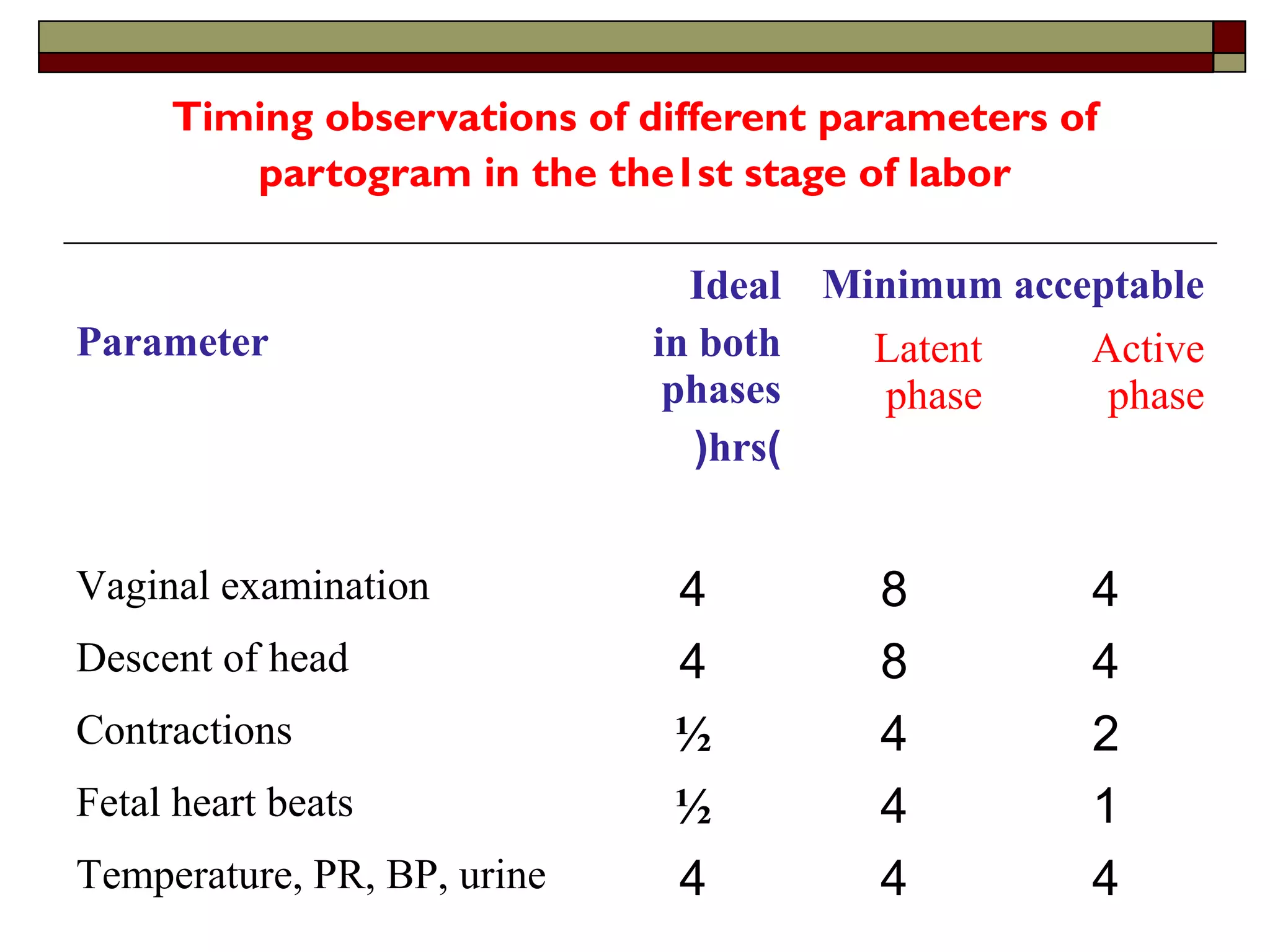
Timing observations ofdifferent parameters of
partogram in the the1st stage of labor
Parameter
Ideal
in both
phases
(hrs)
Minimum acceptable
Latent
phase
Active
phase
Vaginal examination 4 8 4
Descent of head 4 8 4
Contractions ½ 4 2
Fetal heart beats ½ 4 1
Temperature, PR, BP, urine 4 4 4
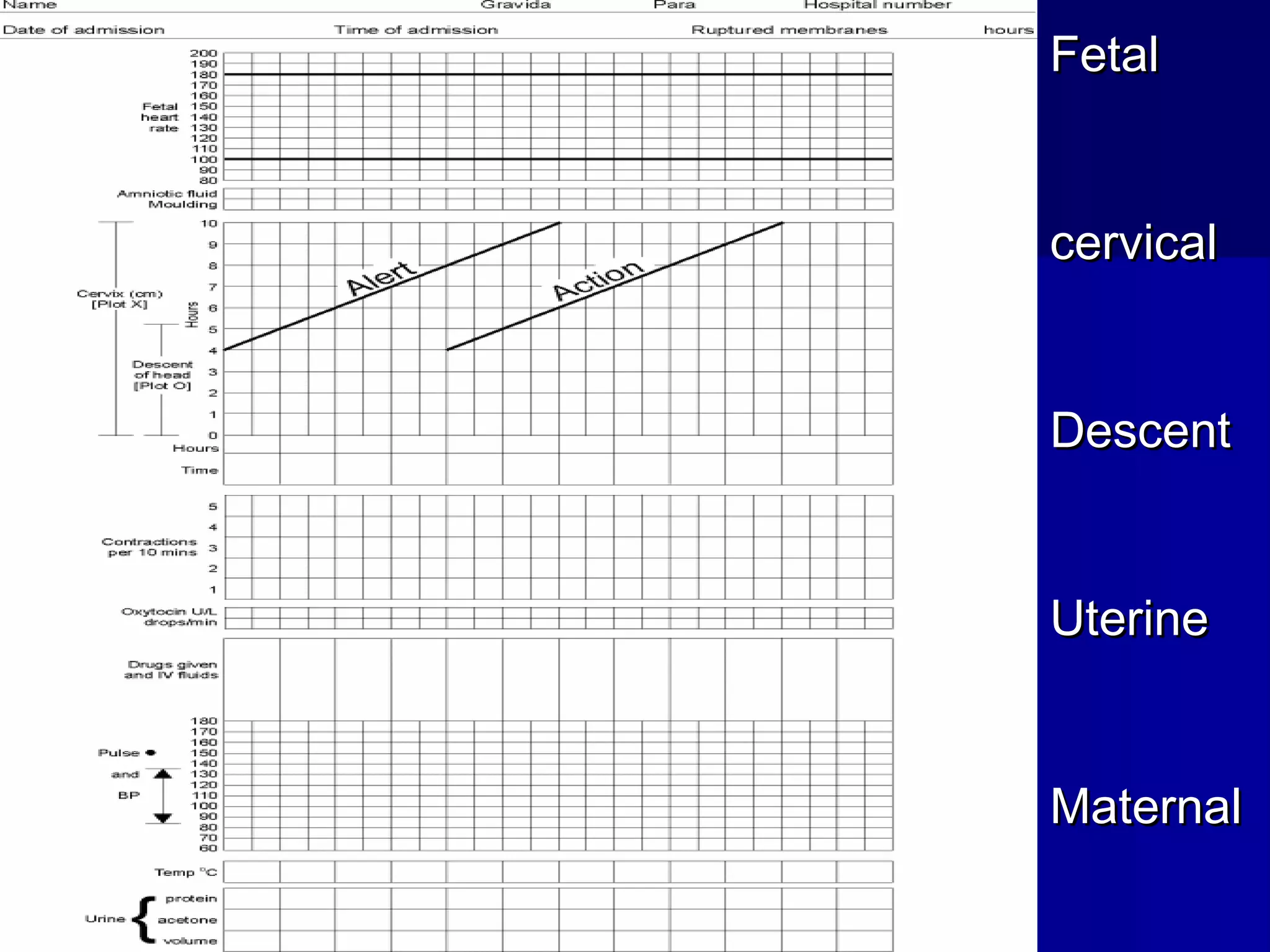
Palpate number ofcontraction in ten
minutes and duration of each contraction in
seconds
• Less than 20 seconds:
• Between 20 and 40 seconds:
• More than 40 seconds:
Management of thirdstage of labour
aimed at:
1-Complete delivery of the after birth
(placenta and membranes).
2-Prevention of acute inversion of the uterus.
3-prevention of postpartum haemorrhage
33.
Delivery of theplacenta and membranes: uterus should
be examined for the presence of second baby
a-Conservative method:
•The left hand is placed just above the fundus to detect any
change in the fundal level, shape and consistency of the
uterus which indicate atony.
• Wait for signs of placental separation and decent,
•Massage uterus to contract
•The patient is asked to bear down to deliver the placenta
spontaneously.
• Ergometrine 0.5mg or Syntometrine(5 units syntocinon +
0.5mg Ergometrine) to be given intravenouslly.
34.
Signs of separationand decent of the
placenta:
1. -The body of the uterus becomes smaller, harder, and
globular.
2. -The fundal level rises in the abdomen because the
lower segment becomes distended by the placenta.
3. -Suprapubic bulge may appear due to presence of the
placenta in the lower segment.
4. -Elongation of the cord out side the vulva.
5. -Sudden gush of blood from the vagina.
35.
b-Active methods (prophylaxisagainst postpartum haemorrhage)
1-Give Methargine 0.5 mg IM or Syntometrine (5units
oxytocin+0.5mg Methargine), at the time of the anterior
shoulder is free from symphysis pubis or as soon as possible
thereafter.
2-Deliver the placenta and membranes by control cord traction by
right hand, and the left hand is placed on the suprapubic
region, pushing the uterus upwards.
N.B. USE SYNTOCINON RATHER THAN METHARGINE
IN CARDIAC AND HYPERTENSIVE CASES.
IV-Post Delivery:
1-examinethe placenta for their completeness, anomalies,
length, and number of vessels in the cord and record the
placental weight.
2-Suture the episiotomy or any laceration.
3-Estimate blood loss, count swabs, and take cord blood for
Hb, blood group, Rh, bilirubin, and coomb’s test for Rh
negative mother.
38.
IV-Post Delivery:
4-CheckBP, P, T, Lochia and firmness of the uterus before
transferring the patient.
5-Continue an infusion of syntocinon through the first hour if
necessary.
6-Allow no food during the first hour, sips of water may be
taken, encourage nursing.