2. • Meningococcemia is defined as dissemination of
meningococci (Neisseria meningitides) into the
bloodstream
• Patients with acute meningococcemia may present
with
• (1) meningitis ( 30%-50%)
• (2) meningitis with meningococcemia (40%)
• (3) meningococcemia without clinically apparent
meningitis (7%-10%)
3. Background
• Neisseria meningitidis is an encapsulated
gram-negative diplococcus
• There are at least 13 serogroups of the
bacterium
• Transmission:
The human nasopharynx is the only known
reservoir for N meningitides, transmitted
via aerosols and nasopharyngeal secretions
5. Pathophysiology
• Endotoxin, cytokines, and free radicals
damage the vascular endothelium,
producing platelet deposition and vasculitis
• Multiple organ failure, shock, and death
may results due to Disseminated
intravascular coagulation (DIC)
7. clinical presentation
• include any of the following:
• A nonspecific prodrome of cough, headache, and
sore throat
• Fever and chills
• malaise, weakness, myalgias, headache, nausea,
vomiting, and arthralgias
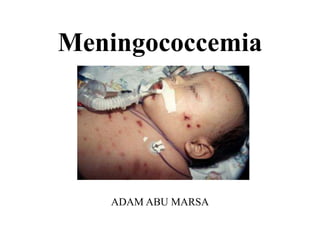
• characteristic petechial skin rash is usually
located on the trunk and legs and may rapidly
evolve into purpura
8. clinical presentation
• Meningitis S&S: Headache, Fever,
Vomiting, Photophobia, Lethargy, Neck
stiffness
• In fulminant meningococcemia, a
hemorrhagic eruption, hypotension, and
cardiac depression, as well as rapid
enlargement of petechiae and purpuric
lesions
9. Physical findings may include the
following:
• Dermatologic manifestations: Petechiae, rash, ecchymoses,
purpura
• Meningococcal meningitis: Pain and resistance to neck
flexion, other signs of meningeal irritation, petechiae, fever
(of variable intensity)
• Meningococcal septicemia: Fever, rash, tachycardia,
hypotension, cool extremities, initially normal level of
consciousness
• Fulminant meningococcemia: Purpuric eruption,
hemorrhages on buccal mucosa and conjunctivae, no signs
of meningitis, cyanosis, hypotension, profound shock, high
fever, pulmonary insufficiency
10.
11.
12.
13.
14.
15. Diagnosis
• Definitive diagnosis of meningococcal disease is
established by isolation of N. meningitidis from a normally
sterile body fluid such as blood, CSF, or synovial fluid
• CBC, electrolytes, coagulation studies, Blood urea nitrogen
and creatinine, Lumbar puncture and CSF analysis, blood
culture
16. PROGNOSIS
• Most deaths occur within 48 hr of hospitalization in children with
meningococcemia
• Poor prognostic factor:
hypothermia or extreme hyperpyrexia,
hypotension or shock,
purpura fulminans,
seizures,
leukopenia, thrombocytopenia (including DIC),
acidosis,
and high circulating levels of endotoxin and TNF-α
• poorer prognosis:
The presence of petechiae for <12 hr before admission, absence of
meningitis, and low or normal ESR
17. Management
• Third-generation cephalosporins such as
ceftriaxone (2 g IV /24h) or cefotaxime (2 g IV
q4-6h) are the preferred antibiotics
• Alternative agents include
• (1) ampicillin 12 g/d either by continuous infusion
or by divided dosing q4h
• (2) moxifloxacin 6-8 g/d IV
• The course of therapy is 7-10 days